1. Stomach
!
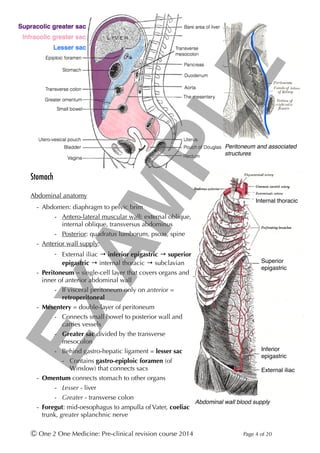
Abdominal anatomy
- Abdomen: diaphragm to pelvic brim
- Antero-lateral muscular wall: external oblique,
internal oblique, transversus abdominus
- Posterior: quadratus lumborum, psoas, spine
- Anterior wall supply:
- External iliac → inferior epigastric → superior
epigastric → internal thoracic → subclavian
- Peritoneum = single-cell layer that covers organs and
inner of anterior abdominal wall
- If visceral peritoneum only on anterior =
retroperitoneal
- Mesentery = double-layer of peritoneum
- Connects small bowel to posterior wall and
carries vessels
- Greater sac divided by the transverse
mesocolon
- Behind gastro-hepatic ligament = lesser sac
- Contains gastro-epiploic foramen (of
Winslow) that connects sacs
- Omentum connects stomach to other organs
- Lesser - liver
- Greater - transverse colon
- Foregut: mid-oesophagus to ampulla of Vater, coeliac
trunk, greater splanchnic nerve
Ⓒ One 2 One Medicine: Pre-clinical revision course 2014 Page ! of !4 20
Peritoneum and associated
structures
Abdominal wall blood supply
External iliac
Inferior
epigastric
Superior
epigastric
Internal thoracic
EXAMPLE
2. - Midgut: to ⅔rd transverse colon,
superior mesenteric artery, lesser
splanchnic nerve
- Hindgut: to dentate line (rectum),
inferior mesenteric artery, least
splanchnic nerve
!
Stomach
- Anterior: diaphragm, transverse colon,
liver
- Posterior: pancreas, spleen, kidney
- Supply: right & left gastric,
gastroepiploic, short gastric [splenic
runs posterior]
- Drain to splenic and superior
mesenteric veins
- Extra (external) oblique muscle layer
- Functions:
- Store & regulate release
- Protein & vit B12 digestion
- Immune defence
- Cephalo-gastric and gastro-gastric
reflexes inhibit vagal contraction to
fill without pressure rise
- Rugae also help filling
without pressure increase
Ⓒ One 2 One Medicine: Pre-clinical revision course 2014 Page ! of !5 20
GIT embryology
Stomach anatomy
Coeliac axis
branches
EXAMPLE
3. Lower oesophageal sphincter
- Competent if sphincter pressure exceeds gastric pressure, contributing factors:
- Muscular (physiological) sphincter itself
- Increase in intra-abdominal/-thoracic pressure with coughing, talking, exhalation
- Acute angle between oesophagus & stomach with mucosal flaps
- Gravity relatively minor role
- Gastro-oesophageal reflux disease (GORD): pain, cough, regurgitation
- Chronic oesophagitis may give Barrett's metaplasia (to gastric type)
- Increased cancer risk
Gastric physiology
- Parietal cells secrete H+ via proton pump (H+-
ATPase) made by carbonic anhydrase (on H2O) +
CO2)
- Target for proton pump inhibitors (e.g.
omeprazole)
- Basolateral HCO3
- excretion (for Cl-) makes alkaline
tide
- Control:
- Vagal innervation of parietal cells increases
directly
- Indirectly: via gastrin from G-cells and
binds CCKB-receptor on parietal cells
- Gastrin reduced by secretin (from duodenal S-cells in response to acid)
- Histamine (ECL cells) increases acid production at H2-R on parietal cells
- Target for histamine antagonists (e.g. ranitidine)
- Somatostatin inhibits directly on parietal cells
- Indirectly: via reducing histamine production from ECL cells
- Mucus increased by ACh (therefore at same time as acid) using PGE2
- Use of NSAIDs reduce PG production and predisposes to gastritis/ulcers
Ⓒ One 2 One Medicine: Pre-clinical revision course 2014 Page ! of !6 20
Gastric acid secretion
Cell type Secretions Function
Parietal cells Gastric acid and
intrinsic factor
Denature protein, immune protection, pepsinogen
activation
Chief cells Pepsinogen Protein digestion
APUD (amine
precursor uptake
decarboxylase) cells
Somatostatin Inhibit acid and increase mucus production
G-cells Gastrin Increase acid production
Mucus-secreting cells Alkaline mucus Protect epithelium from acid-damage
ECL (entero-
chromaffin-like) cells
Histamine Increase acid production
EXAMPLE
4. - Gastric motility
- Mixing in corpus
- Propulsion moves towards
antrum
- Retropulsion back from
antrum/pylorus to corpus
- Pylorus relaxes in response
to: distention, small boluses,
peptides
!
Small bowel
!
Anatomy
- Duodenum: superior (coeliac) &
inferior (SMA) pancreato-duodenal
arteries
- Posterior to 1st: common bile
duct, gastroduodenal artery and
portal vein
- Posterior to 2nd: right kidney and
ureter
- 3rd: around head of pancreas,
crossed by root of the
mesentery & SMA
- 4th: ligament of Trietz at
duodeno-jejunal junction with
IMV to left
- Histology:
- Brunner's glands: deep, alkaline-secreting, only in duodenum
Ⓒ One 2 One Medicine: Pre-clinical revision course 2014 Page ! of !7 20
Helicobacter pylori
- Bacterium specialised to living in stomach
- Associated with peptic ulcer disease
- Urease produces an alkaline coat
- Flagella to bury into mucus
- Inhibits somatostatin secretion → increases acid
Control of gastric acid
Duodenal anatomy
EXAMPLE
5. - Simple columnar with microvilli
- Jejunum (2/5th): thicker with smaller lumen
- Plicae circulares (/valvulae conniventes) = folds in small bowel
- Villae (= mucosae) with crypts of Leiberkuhn at base (new cells produced at base)
- Peyer's patches = lymphoid aggregates
- B-cells make secretory IgA that prevent pathogen adhesion
- Panneth cells secrete lysozyme
!
!
!
!
!
!
!
!
!
!
Absorption
!
Water & ions
- Basolateral Na+/K+-ATPase gives concentration gradient for apical facilitated diffusion:
co-transport with glucose, amino acids and chloride
- Water via osmosis through leaky occluding junctions in upper GIT and small bowel
- Large bowel through aquaporins and transcellular movement
- More controlled
- K+ and Cl- move by paracellular transport; plus H+/K+-ATPase absorbs K+ in colon
!
Ca2+
- Facilitated uptake in duodenum - binds calbindin inside cells (keeps gradient)
- Basolateral efflux by Ca2+-ATPase or Na+/Ca2+-antiporter
- PTH increases channel activity and vitamin D increases calbindin synthesis
!
Ⓒ One 2 One Medicine: Pre-clinical revision course 2014 Page ! of !8 20
- Peritoneal cavity has a greater and lesser sac, separated by the
stomach and it’s attachments
- Mesentery is double-layered peritoneum containing neurovascular
supply
- Gastric parietal cells produce acid using H+/K+-ATPase
- Duodenum is retroperitoneal and is both fore- & mid-gut
Sodium & water absorption in the
small bowel
EXAMPLE
![- Midgut: to ⅔rd transverse colon,
superior mesenteric artery, lesser
splanchnic nerve
- Hindgut: to dentate line (rectum),
inferior mesenteric artery, least
splanchnic nerve
!
Stomach
- Anterior: diaphragm, transverse colon,
liver
- Posterior: pancreas, spleen, kidney
- Supply: right & left gastric,
gastroepiploic, short gastric [splenic
runs posterior]
- Drain to splenic and superior
mesenteric veins
- Extra (external) oblique muscle layer
- Functions:
- Store & regulate release
- Protein & vit B12 digestion
- Immune defence
- Cephalo-gastric and gastro-gastric
reflexes inhibit vagal contraction to
fill without pressure rise
- Rugae also help filling
without pressure increase
Ⓒ One 2 One Medicine: Pre-clinical revision course 2014 Page ! of !5 20
GIT embryology
Stomach anatomy
Coeliac axis
branches
EXAMPLE](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)