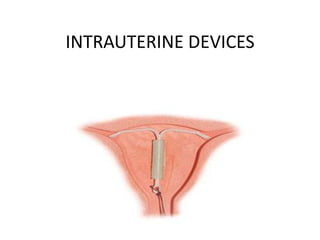
2. INTRODUCTION AND HISTORY
• IUDs are one of the way of long term contraceprion.
• used by 15% of women world wide, in INDIA its 11%.
• The IUD has had a troubled history.
• Its survival has been jeopardized several times from the beginning.
• first genuine IUD was devised by Dr Richter in 1909- consisting
of silkworm catgut ring with a nickel and bronze wire protruding
through cervix, shortly Pust modified the design he combined
the ring with button type passary and rplaced the wire with
catgut, this IUD was used in Germany during world war II.
•In 1920s Grafenberg removed tail and pessary as he belived
that it causes infection.
• Grafenberg’s ring was associated with high expusion rate.
cont…
3. • Further many modifications were made as far as size and shape
and material is concerned to minimize side effects.
• In the 1960s it was 1st time when plastic devices were developed
impregnated with barium, The Margulies coil devised by Lazer
Margulies was the 1st plastic devise with a memory, which allow
the use of inserter and reconfiguration of shape in uterus, the coil
was large associated with bleeding and cramping and was
withdrawn.
• In 1962 Dr J.Lippes presented his experience with his device in
front of 1st international conference ‘Lippes loop’
which quickly became most widely used IUD.
• Further many designs came in between but the addition of
copper to IUD was suggested by Dr. Jaime Zipper whose
experiments indicate that Cu acted locally on endometrium.
• It was Haward Tatum who combined this idea with development
of T-shape, 1st copper containing IUD was Cu T 200, also called as
Tatum-T.
•Followed by further modification to increase efficacy and life
span and recently medicated IUD are introduced.
4. Types of IUDs
Classification
• Non medicated IUDs
Lippes loop
• Medicated copper containing IUDs
Cu T 200, Cu T 380 A, Multiload250, Multiload-375, Nova T.
• Hormone containing IUDs
LNG-20
8. MECHANISM OF ACTION
Non medicated IUDs –
Leads to foreign body reaction (produces
sterile inflammatory response) which is
spermicidal.
Copper IUDs-
Leads foreign body reaction & in addition
produces alteration in cervical mucus &
endometrial secretion, and initiates release
of cytokine peptides known to be cytotoxic.
Hormone containing IUD- Levonorgestrel IUD suppresses
endometrium leading to atrophy &
thickens cervical mucus hindering
penetration
9. Characteristics of IUDs
• Highly effective and economical
• No interference with intercourse
• Easy to us
• Long acting
• Locally acting
• easily reversible and quick return to
fertility
10. Copper containing IUDs
• Cu T 200
Contains 200 sq mm surface area of wire
containing Cu.
Cu wire wounded round the vertical
stem, T shaped frame made of Polyethylene, with
polyethylene threads.
life span is 3 years
Failure rate 3%
• Replaced by modern copper IUDs containing
more copper with increased efficacy and life span.
11. Cu T 380 A
• Holds 380 mm2 of Cu, wire wounded
on stem with extra copper sleeves on
both arms of T.
• “A” indicates Arms, indicating
importance of copper sleeve on each
arm with introduction of sleeves
efficacy and lifespan is increased.
• life span 10 yrs
• failure rate- 0.3 to 0.8 per HWY
• further ball at the bottom of stem
reduce risk of perforation and reduces
cramp like pain
12. LNG-20
LNG-20 consists of a T-shaped
polyethylene frame (T-body) with a
steroid reservoir around the vertical stem.
The reservoir made of a mixture of
levonorgestrel and silicone containing a
total of 52 mg levonorgestrel. The
reservoir is covered by a semi-opaque
silicone membrane. The T-body is 32 mm
in both the horizontal and vertical
directions. The polyethylene of the T-body
is compounded with barium sulfate.
The reservoir releases 20mcg per day
which declines to half rate after 5 years.
Life span- 5 yrs in USA & 7 yrs in Europe
and Asia( has to be changed)
Failure rate-0.1 to 0.2 per HWY
cont…
13. Other uses of LNG 20
1) Extensively used to treat Heavy menstrual bleeding as n
alternative to hysterectomy.
2) Has beneficial effect in menorrhagia from uterine
fibroid, benefit may be diminished with distorting sub
mucosal fibroid.
3) The local Progestin effect directed to endometrium can
be utilized in patients on tamoxifen, and in women
receiving estrogen therapy.
4) Reduces risk of Ca endometrium
5) Improvement in symptoms of endometriosis and
adenomyosis.
14. Who can use IUDs
Can be safely used by women who:
• are of various age and parity (young and nulliparous
women should told about expulsion risk.
• are post partum, post abortion of breast feeding.
• have chronic condition, including
Hypertension, cardiovascular disease, diabetes, liver &
gall bladder disease.
15. Contraindications of IUD
• Pregnancy
• Puerperal sepsis
• PID
• STDs current or within the past 3 months
• Endometrial or cervical cancer
• undiagnosed genital bleeding
•Uterine anomalies
•Fibroid tumors distorting the endometrial cavity
• Copper allergy and wilson’s disease
Infection with HIV no more contraindication for IUD use as no
increase in PID, Female to male transmission, or viral shedding
was found among HIV-1 infected women.
16. Time of Insertion
• IUDs can be safely inserted at any time after
Delivery ( Normal or Cesarean)
Abortion ( spontaneous or induced)
or during the menstrual cycle.
• Expulsion rate were higher when the older, large plastic IUDs
were inserted sooner than 8 weeks
but Cu T can be inserted between 4 to 8 weeks
postpartum without an increase in pregnancy
rates, expulsion, uterine perforation, or removal from bleeding
and/or pain.
• Post delivery insertion
NOT associated with infection, perforation, PPH, or sub
involution, but associated with slightly higher expulsion rate as
compare with insertion 4-8 weeks.
Cont…….
17. • IUDs can also be inserted at cesarean section; the expulsion
rate is slightly lower than with insertion immediately after
vaginal delivery.
• IUDs can be inserted after 1st trimester abortion but after 2nd
trimester it is recommended to wait until uterine involution
occurs.
• Post menstrual insertion- advantage of open cervical canal
and masking of insertion related bleeding
further evidences support that expulsion
rate, termination rate, bleeding and pregnancy are lower if
insertion is performed after day 11 of menses, and infection
rate may be lower with insertion after 17th cycle day.
18. Screening the patient before IUD insertion
• Age and parity are not the critical factors in selection, most of
the women are good candidate for IUD.
• Pregnancy to be ruled out.
• Detail history pertaining to sign and symptoms suggestive of
PID to be elicited as any current, recent or recurrent PID is a
contraindication for IUD use.
• High risk behavior, women with multiple sexual partner, drug or
alcohol dependent, not in stable sexual relationship are at greater
risk of PID at the time of insertion and at greater risk of acquiring
a STD after IUD insertion.
cont……
19. • Ideal choice for a women with diabetes, specially if vascular
disease is present.
•Not contraindicated in Heart diseases, patient at risk of
endocarditic should be treated with prophylactic antibiotics.
• A careful PS and bimanual examination is must
- position of uterus; undetected extreme posterior
position is most common reason for perforation.
- A very small or large uterus can preclude insertion, for
successful use, the uterus should preferably not sound less than
6cm or more than 9cm.
- also helps to rule out cervical or vaginal infection and
any bleeding though OS.
20. ADVICE after insertion
• Protection against unwanted pregnancy begins
immediately after insertion.
• Menses can be longer and heavier (except with hormonal
IUDs)
• IUDs can be spontaneously expelled; monthly palpation of
the strings is important, If a string are not felt clinician to be
notify further backup contraception should be provided until
patient can be examined.
21.
22.
23.
24. Infections
• IUD related bacterial infection are due to contamination of
cavity at time of insertion.
• The early insertion related infections therefore, are
polymicrobial, and derived from endogenous cervicovaginal
flora, with predominance of anaerobes.
• As per WHO clinical trial data, risk of PID is 6 times higher
during 20 days after the insertion compared with later times
during follow up, but most importantly PID is extremely rare
beyond the first 20 days after insertion.
• Risk of PID does not increase with long term use.
• The sexual behavior of the patient is one of the strong
modifier of the risk of infection- advice a barrier contraception
in addition to IUD
Cont……
25. Prevention of Infections
• The problem of infection can be minimized with careful
screening and by following aseptic techniques.
•Doxycycline 200mg or Azithromycin 500 mg orally 1 hour
prior to insertion provide protection against PID, but are
probably of little benefit for women at low risk for STIs.
•IUDs are not contraindicated in women who are at
increased risk of bacterial endocarditis
• antibiotic prophylaxis of 2 gm amoxyxillin should be given
1 hour prior before insertion or removal.
26. Treatment of Infections
• Asymptomatic IUD users whose cervical cultures showing
growth of Gonorrheal or Chlamydia infection should be treated
without removal of IUD.
• vaginal bacteriosis should be treated without removal of IUD
unless pelvic infection is present.
•If infection has spread to endometrium, or fallopian tubes IUD
should be removed promptly with specific medical management.
• If infection is sever as evidence by cervical motion
tenderness, abdominal rebound tenderness, adnexal tenderness
or masses, or elevated WBC count, and sedimentation rateparenteral treatment is indicated with removal of IUD
27. HIV and IUDs
• IUDs are not contraindicated in women with HIV
positive status.
• does not increase risk female to male transmission.
• No grater incidence of complication (including
PID).
28. Actinomyces
• Actinomyces are commonly present in vaginal flora.
•The only pelvic infection that was unequivocally related to
IUD use is Actinomycosis.
• Incidence is less than 1% with copper containing IUD.
• symptomatic patients should be treated with
oral Penicillin G 500 q.i.d. for 1 month or Tetracycline 500
mg q.i.d. , Doxy 100 mg b.d , amoxy/clavulanate 500 mg b.d.
29. Bleeding with IUDs
• Most common cause of IUD discontinuation- increased
uterine bleeding and increased pain during menses.
• Bleeding and cramping are most sever in first few months
after IUD insertion- NSAID are helpful during menses.
• Use of copper IUD leads to increase in menstrual blood
loss by about 55%, and this level of bleeding continues for
duration of use, however its no so with LNG-20, it leads to
oligomenorrhea in 70% of women and in 30-40%
amenorrhea (sometimes women wants IUD removal
because of lack of periods).
30. IUDs AND ECTOPIC PREGNANCY
• IUDs do not increase the risk of ectopic pregnancy
however, if pregnancy occurs, the likelihood of an ectopic
pregnancy is high.
• A WHO multicentre study concluded that IUD users were
50% less likely to have an ectopic pregnancy when
compared with women using no contraception.
• This protection is not as great as that achieved by
inhibition of ovulation with oral contraceptive.
• Risk do not increase with duration of use of Cu T 380 A and
LNG-20.
cont….
31. ECTOPIC PREGNANCY RATE PER 1000 women year
Non-contraceptive users, all ages
3.00-4.50
LNG-20
0.20
Cu T 380A
0.20
• In a 7-year prospective study, not a single ectopic pregnancy
was encounter with LNG-20. In 8,000 woman-year of experience
in multicentre trials, there has been only a single ectopic
pregnancy reported with Cu T 380A.
• The protection against ectopic provided by Cu T 380A and LNG20 makes these IUDs acceptable choices for contraception in
women with previous ectopic pregnancy.
32. Pregnancy with IUDs in situ
• Spontaneous miscarriage occurs more who became pregnant
with IUD in situ, a rate of 40 to 50%.
• Remove IUD if pregnancy is confirmed provided string is
visible, use of instruments inside uterus should be avoided.
• after removal spontaneous abortion rate is 30%.
•If IUD is easily removed without trauma or expelled during the
first trimester, the risk of spontaneous miscarriage is not
increased.
Cont….
33. • When the string of IUD is not visible
-Perform an USG to localize IUD and to determine
whether expulsion has occurred.
-if IUD is present, 3 options
1) Therapeutic abortion
2) USG guided removal
3) Continuation of pregnancy with device left in
situ.
• USG guided removal possible when IUD is not in fundal
region, if its in fundal region should be left in situ.
• IUD left in situ with pregnancy has higher incidence (4
fold) of PTLP’s with no evidence of risk of congenital
malformaiton.
34. IUDs and uterine perforation
• 1 in 1000, risk linked to skill and experience of clinician.
• Most perforation occurs at the time of insertion but
migration may occur following initial partial perforation.
•Most perforation go undetected as it leads to transient pain
and bleeding at time of insertion, so in case of doubt
perform USG to detect position of IUD.
•Suspected when no thread is visible through Ext OS with
appearance of pelvic symptoms in women using IUD.
35. •Further Negative findings on exploration of uterine cavity by a
probe is suggestive.
• USG helps in localization of IUD (better than X-ray)
• Cu containing devise if displaced in peritoneal cavity leads to
adhesion formation and should be removed via laparoscopy or
laparotomy.
36. Dealing with missing thread…..
• 3 Possibilities
• Expulsion.
• Displacement (IUD inside uterus but displaced).
• perforation and migration to peritoneal cavity.
• All IUDs are radiopaque, but localization with help of X-ray
needs 2-3 views and does not allow intrauterine direction of
instruments, So USG is best way to locate an IUD.
•If IUD is inside uterus an can be grasping with help of
forceps under USG guidance, if not possible next is
hysteroscopic removal of embedded IUD.
• If IUD is identified perforating myometrium or in the
abdominal cavity to be removed with help of laparoscopy.
• With sighs and symptoms of peritonitis with perforation
laprotomy should be done.
37. IUD as Emergency contraception
• Efficacy for emergency contraception is 100% when the
device is inserted up to 5 days after intercourse.
• and almost 100% up to 7 days after intercourse.
• Best is Cu T 380 A
• Advantage of using Cu T 380 A as emergency
contraception is patient can continue with it for long term
contraception making it cost effective.
• Whether LNG-20 would work for emergency contraception
is not known.