
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Xenobiotic effects on leukocytes
Similaire à Xenobiotic effects on leukocytes (20)
Dernier
Dernier (20)
Xenobiotic effects on leukocytes
- 1. Xenobiotic Effects On Hematopoietic (Leucocytes). Ph. Nisreen Sami Hasab Higher Diploma in Toxicology & Pharmacology Supervised by:- Dr. Ammar Ali Hussein 2020
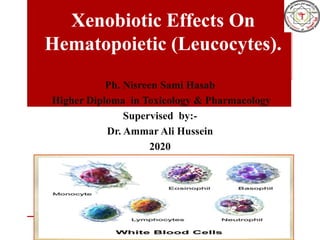
- 2. White Blood Cells (WBCs) or Leukocytes :- leukocytes are far less numerous than red blood cells, they are important to body defense against disease. On average, there are 4000 to 11.000 WBCs/mm3, and they account for less than 1 percent of total blood volume. White blood cells are the only complete cells in blood; that is; they contain nuclei and the usual organelles. Leukocytes form a protective, movable army that helps defend the body against damage by bacteria, viruses, parasites, and tumor cells. As such they have some very special characteristics. White blood cells, by contrast, are able to slip into and out of the blood vessels (by process called diapedesis). WBCs can locate areas of tissue damage and infection in the body by responding to certain chemicals that diffuse from the damaged cells. This capability is called positive chemotaxis.
- 4. Types of WBCs:- WBCs are classified into two major groups, depending on whether or not they contain visible granules in their cytoplasm. Granulocytes :- are granule-containing WBCs. They have lobed nuclei, which typically consist of several rounded nuclear areas connected by thin strands of nuclear material. The granules in their cytoplasm stain specifically with Wright's stain. The granulocytes include the neutrophils, eosinophil and basophils. 1. Neutrophils:- have a multilobed nucleus (3-5lobes) and very fine granules that respond to both acid and basic stains. Consequently, the cytoplasm as a whole stains pink. Neutrophils are avid phagocytes at sites of acute infection.
- 5. 2. Eosinophils :- have a bilobed blue-red nucleus that resembles an oldfashioned telephone receiver and large red cytoplasmic granules. Their number increases rapidly during allergies and infections by parasitic worms (flat-worms, tapeworms, etc.). 3. Basophils :- the rarest of the WBCs, have S shaped nucleus contain large histamine-containing granules that stain dark blue. Histamine is an inflammatory chemical that makes blood vessels leaky and attracts other WBCs to the inflammatory site. AGranulocytes :- lack visible cytoplasmic granules. Their nuclei are spherical oval or kidney-shaped. The agranulocytes include lymphocytes and monocytes .
- 6. 1. Lymphocytes :-have a large dark purple nucleus that occupies most of the cell volume. Only slightly larger than RBCs, lymphocytes reside in lymphatic tissues, where they play an important role in the immune response. There are two types of lymphocytes: • T lymphocytes: provide cell mediated immunity.mature in the thymus. • B lymphocytes: provide humoral immunity. • Natural killer cells (NK cells) :NK cells arise from lymphoid precursor cells, but receptors can be activated with or without binding antibodies or a major histocompatibility complex. Detection and destruction of cells that do not express MHC-I receptors.Cells infected with viruses (especially herpes viruses)Tumor cells Kill via : Induction of apoptosis (granzymes, perforin) Antibody-dependent cell-mediated cytotoxicity (activated by binding of CD16) Cytokine production: INF-γ and TNF-α ,Function enhanced by IFN-α and IFN-β, IL-2, IL-12
- 7. 2. Monocytes:- are the largest of the WBCs. Except for their more abundant cytoplasm and indented (kidney like) nucleus, they resemble large lymphocytes. When they migrate into the tissues, they change into macrophages. Macrophages are very important in fighting chronic infections, such as tuberculosis. The granulocytes and the monocytes protect the body against invading organisms by ingesting them by the process of phagocytosis. The lymphocytes function mainly in connection with the immune system. However, a function of certain lymphocytes is to attach themselves to specific invading organisms and destroy them.
- 8. Genesis of the Leukocytes :-two major lineages of white blood cells are also formed, the myelocytic and the lymphocytic lineages. The lymphocytic lineage beginning with the lymphoblast; that produce lymphoctes, and the myelocytic lineage beginning with the myeloblast; which produce other WBCs. The granulocytes and monocytes are formed only in the bone marrow. Lymphocytes are produced mainly in the various lymphogenous organs, including the lymph glands, the spleen, the thymus, the tonsils, and various lymphoid rests in the bone marrow, gut, and elsewhere. These colony stimulating factors (CSFs) and interleukins not only prompt red bone marrow to turn out leukocytes, but enhancing the ability of mature leukocytes to protect the body. Apparently, they are released in response to specific chemical signals in the environment such as inflammatory chemicals and certain bacteria or their toxins.
- 10. Xenobiotics: Sources and Types:- Originally, the term xenobiotic comes from the Greek word xenos , which means foreign or strange, and ‘bios’, which means life. Xenobiotics are chemical compounds exhibiting abnormal structural characteristics . The unusual presence of any substance in high concentrations, the presence of antibiotic drugs in the human body which may not be produced by the body itself nor is a normal part of diet. At times, a natural substance can be defined as a xenobiotic if it found its way into humans or other animals. -Bonjoko (2014) proposed the word ‘xenobiotic’based on the physiological and biological effects of exogenous substances whether natural or synthetic (drugs, chemicals) on the cells, tissues or organs of the organisms. Many xenobiotics are potientially hazardous to the organisms which are exposed to them in the environment . Xenobiotics may persevere for long term (months to years) in the environment. For example, the polymer structure of lignin .
- 11. antithyroids, anticonvulsants, chemotherapy, sulfas or other antibiotics, analgesic, drugs used in Immune dysfunction(AIDS, rheumatoid arthritis), etc . Medications X_ray media ,free radical that increase oxidative stress . Radiation. alcohol, benzenes.Toxins Cadmium, Lead (Pb), Mercury (Inorganic), Arsenic.Heavy metals Pesticides such as fungicides, herbicides and rodenticides . Organophosphate and organochlorine insecticides (synthetic pesticides). Environment pollution or industrial
- 12. Drug-Induced agranulocytosis:- Agranulocytosis is defined as a reduction in the number of mature myeloid cells in the blood (granulocytes and immature granulocytes ) to a total count of 500 cells/mm3 (0.5 × 109/L) or less. In Europe, the incidence rate is reported to range from 1.6 to 9.2 cases per million population. In the United States, reported rates are slightly higher, ranging from 2.4 to 15.4 cases per million population. Geographic variability in incidence is related to both differences in reporting and medication usage but could also suggest genetic differences in susceptibility. Older patients are thought to be at greater risk for to drug-induced agranulocytosis, probably because of increased medication use. Drug-induced agranulocytosis also occurs more frequently in women than in men. The mortality rate is highest among elderly adults and patients with renal failure, bacteremia, or shock at the time of diagnosis. Symptoms of agranulocytosis arise from the increased infection risk associated with the lack of WBCs and include sore throat, fever, malaise, weakness, and chills. Symptoms may appear either immediately or insidiously, depending on the time course of neutropenia development.
- 13. Symptoms may appear either immediately or insidiously, depending on the time course of neutropenia development. The median duration of exposure before the development of agranulocytosis ranges from 19 to 60 days for most drugs associated with this adverse event, but the time to onset is greater than 1 month for most of these agents. The cause of drug-induced agranulocytosis is not fully understood, but two mechanisms—direct toxicity and immune-mediated toxicity—have been proposed. Direct toxicity to myeloid cells, particularly neutrophils, has been shown with medications such as:- chlorpromazine, procainamide, clozapine, dapsone , sulfonamides, carbamazepine, phenytoin, indomethacin, and diclofenac . The toxicity may be due to either the parent drug or a toxic metabolite or by product. The severity of neutropenia associated with these drugs is often dose dependent, but the occurrence of reactions is still idiosyncratic
- 14. Within the immune-mediated subset of agranulocytosis, there are three proposed mechanisms of toxicity. The hapten mechanism involves the drug or its metabolite binding to the membrane of neutrophils or myeloid precursors. After binding, antibodies are induced that destroy the cell. This is thought to be the mechanism of agranulocytosis induced by aminopyrine, penicillin, and gold compounds.
- 15. In the immune-complex mechanism, antibodies form complexes with the causative drug, and the immune complex adheres to the target cell, leading to cell destruction. This is the proposed mechanism of agranulocytosis induced by quinidine and quinine . The drug induces antibody formation. The antibodies and drug form a complex in the serum, and the complex nonspecifically binds to the cell membrane. Complement is activated, and the cell is lysed.
- 16. Protein carrier mechanism. The drug combines with a plasma protein. The complex then attaches to the cell membrane, and antibody formation is stimulated. Antibodies later attach to the complex and activate complement. The cell is then lysed by the complement. Nearly all classes of drugs have been associated with some incidence of acute neutropenia or agranulocytosis, although the risk is exceedingly small. For some drugs, though, the risk may be higher. These agents include antithyroid medications, sulfasalazine, trimethoprim–sulfamethoxazole, and β-lactam antibiotics.
- 17. Treatment--Drug-Induced agranulocytosis:- The primary treatment of drug-induced agranulocytosis is the removal of the offending drug. After discontinuation of the drug, most cases of neutropenia resolve over time, and only symptomatic treatment (e.g., antimicrobials for infection treatment and prophylaxis). Sargramostim (granulocyte-macrophage colony-stimulating factor [GM-CSF]) and filgrastim (granulocyte colony-stimulating factor [G-CSF]) have been shown to shorten the duration of neutropenia, length of antibiotic therapy, and hospital length of stay. A commonly reported regimen is G-CSF 300 mcg/day via subcutaneous injection.
- 18. Leucopenia :- A range of disorders can cause decreases in white blood cells. This type of white blood cell decreased is usually the neutrophil. In this case the decrease may be called neutropenia or granulocytopenia. Less commonly, a decrease in lymphocytes (called lymphocytopenia or lymphopenia). Neutropenia :- can be acquired or intrinsic. A decrease in levels of neutrophils on lab tests is due to either decreased production of neutrophils or increased removal from the blood. The following list of causes is not complete. • Medications - chemotherapy, sulfas or other antibiotics, phenothiazenes, benzodiazepines, antithyroids, anticonvulsants, quinine, quinidine, indomethacin, procainamide, thiazides. • Radiation. • Toxins - alcohol, benzenes. • Intrinsic disorders - Fanconi's, Kostmann's, cyclic neutropenia. • Immune dysfunction - disorders of collagen, AIDS, rheumatoid arthritis. • Blood cell dysfunction - megaloblastic anemia, myelodysplasia, marrow failure, marrow replacement, acute leukemia. • Any major infection.,Miscellaneous - starvation, hypersplenism.
- 19. Lymphocytopenia:- Defined as total lymphocyte count below 1.0x109/L, the cells most commonly affected are CD4+ T cells. Like neutropenia, lymphocytopenia may be acquired or intrinsic and there are many causes. One causes Medications - chemotherapy (antilymphocyte globulin therapy, alemtuzumab,glucocorticoids),Radiation. Leukocytosis:- An increase in the number of white blood cells in circulation is called leukocytosis. Neutrophilia :- Neutrophilia is an increase in the absolute neutrophil count in the peripheral circulation. Normal blood values vary by age. Neutrophilia can be caused by a direct problem with blood cells (primary disease). It can also occur as a consequence of an underlying disease (secondary). One cause :- Cigarette smoking – occurs in 25–50% of chronic smokers and can last up to 5 years after quitting. Medication induced – corticosteroids (for example, prednisone, β-agonists, lithium) Cancer – either by growth factors secreted by the tumor or invasion of bone marrow by the cancer.
- 20. Eosinophilia :- A normal eosinophil count is considered to be less than 0.65×109/L .Eosinophil counts are higher in newborns and vary with age, time (lower in the morning and higher at night), exercise, environment, and exposure to allergens. Eosinophilia is never a normal lab finding. Lymphocytosis :- Increase in number of lymphocytes in the blood to > 4000/μL (absolute) or > 50% of all leukocytes causes by Acute viral infections (e.g., rubella, infectious mononucleosis, mumps) Neoplasia (e.g., Hodgkin lymphoma, non-Hodgkin lymphoma, chronic lymphoid leukemia) ,Chronic infections (e.g., tuberculosis, syphilis, toxoplasmosis)
- 21. Conclusion:- Keywords Xenobiotics • Carcinogens • Degradation Environmental contamination by xenobiotics is a worldwide phenomenon as a result of human activities resulting from rise in urbanization and population growth. There are numerous sources of xenobiotics ranging from pharmaceuticals to agriculture. In addition, the making of unlawful drugs has led to the discharge of harmful carcinogens into the water system. The release of these harmful pollutants results in numerous short- and long-term effects to the natural ecosystem. Since the time of the Industrial Revolution, scientific and technological permitted humans in the over utilization of resources creating disturbance to the natural ecosystem. The generation of huge amount of toxic substances released from industrial caused widespread contamination of the ecosystem. The major contaminants are halogenated and nitrated hydrocarbons ,Several herbicides, insecticides and fertilizers.
- 22. References :- 1-Ninth Edition Lewis S. Nelson, MD, Neal A. Lewin, MD, Mary Ann Howland, PharmD, Robert S. Hoffman, MD, Lewis R. Goldfrank, MD, Neal E. Flomenbaum, MD, 2015. 2- Coates TD. Drug-Induced Neutropenia and Agranulocytosis. In: Post TW, ed. UpToDate. Waltham, MA: UpToDate. https://www.uptodate.com/contents/drug- induced-neutropenia-and-agranulocytosis. Last updated August 1, 2016. Accessed May 7, 2017. 3- Environmental Xenobiotics and Its Effects on Natural Ecosystem , All content following this page was uploaded by Asha Embrandiri on 07 March 2019 this publication at: https://www.researchgate.net/publication/311978744 .