Electrophoresis
•
13 j'aime•7,673 vues

notes on electrophoresis, useful for postgraduate medical and paramedical students

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Electrophoresis
Similaire à Electrophoresis (20)
Plus de Ashish Jawarkar
Plus de Ashish Jawarkar (20)
Dernier
Dernier (20)
Electrophoresis
- 1. 1 ELECTROPHORESIS Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 2. 2 OVERVIEW 1. History 2. Zonal electrophoresis Principle Method 3. Buffer 4. Support media 5. Ancillary techniques before performing electrophoresis Precipitation Column separation - Gel filteration - Ion exchange chromatography (anion exchange, cation exchange) - Hydrophobic chromatography - Affinity chromatography - Capillary electrophoresis 6. Summary of workflow 7. Applications a. Serum protein electrophoresis b. CSF electrophoresis c. Urine electrophoresis d. Hemoglobin electrophoresis Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 3. 3 * HISTORY 1. The technique of electrophoresis was introduced by Tiselius. 2. His technique is known as MOVING BOUNDARY ELECTROPHORESIS / FRONTAL ELECTROPHORESIS 3. He separated proteins dissolved in electrolyte solution by application of electric current through U shaped quartz tube that held the solution. 4. At ph 7.6, the solution got separated into four distinct protein fractions, albumin, α, β and γ. These separated proteins were identified by checking the change in refractive index across the solution. 5. As there was no solid support to the medium, these separated proteins did not form distinct zones. Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 4. 4 * ZONAL ELECTROPHORESIS 1. In Teselius’ technique, the proteins cound not form distinct bands 2. This problem was solved by introducing an anticonvection solid support medium – like filter paper. 3. Now on applying electric current, the proteins separated into discrete bands at ph 8.6 4. The α band got further split into α1 and α2. 5. Other solid media that are frequently used nowadays include cellulose acetate membrane, agarose gel, starch gel and polyacrideamide gel. Anode Cathode Principle: 1. The proteins to be separated are applied at anode. 2. The support medium has negative charge – the electromotive force (determined by charge of proteins and pH) tends to move the support medium towards anode (positive pole) – but support medium cannot move. 3. The buffer ions have positive charge – they tend to move towards cathode. 4. This net result is flow of buffer towards cathode – this force called electro osmotic force (endosmosis). 5. The buffer ions carry with them water molecules and protein molecules. Proteins here move not only on the basis of their charge, but also determined by their molecular weight. 6. This explains the movement of slightly negatively charged γ globulins towards the cathode. 7. The actual distance traveled by the protein is dependent on these two forces described above. Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 5. 5 Method: 1. The sample to be separated is soaked into a gel. 2. Each end of the gel is then inserted into separate buffer chambers in which electrodes are mounted. 3. An electric current is then passed through the gel for a period of, about 30 minutes usually. 4. After this the gel is treated with a mild fixative such as acetic acid. 5. This fixative precipitates the proteins at the positions on the gel to which they have migrated to. 6. They are then stained and the gel is dried. 7. The protein patterns can now be visually inspected for qualitiative identification of abnormal proteins. 8. To find out the quantity of each type of protein present, densitometric scanners are used, they generate tracings and quantitate relative percentages of proteins in each fraction. 9. These percentages when multiplied by total proteins can give an idea about the concentration of protein in each fraction. Eg. If total protein is 9 gm/dl and albumin fraction obtained is 50% - = 4.5 gm/dl (9 x 50/100) is the albumin concentration 10. On varying the buffer media / solid media – different applications of electrophoresis can be developed. Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
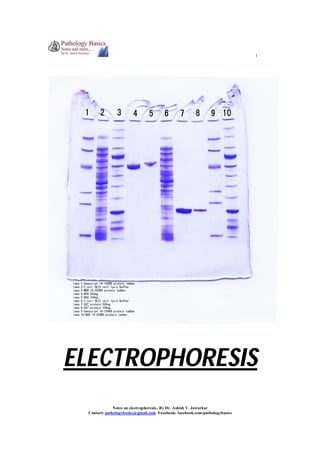
- 6. 6 * Varying buffer concentration and its application 1. If endosmosis is set at a high, this maximizes cathodal movement. 2. Immunoglobulins can be separated optimally and this helps in detecting oligoclonal bands in CSF Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 7. 7 * Varying solid media and its applications PAGE – Polyacrylamide Gel Electrophoresis 1. Polyacrylamide is an inert support medium 2. It is useful for standard separation of native proteins based on charge Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 8. 8 SDS-PAGE – Sodium dodecyl sulphate Polyacrylamide gel electrophoresis 1. SDS denatures proteins according to their molecular weight 2. SDS-PAGE is very powerful for resolving proteins and separating them into subunits according to their molecular weight 3. Very useful for research purposes Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 9. 9 TWO DIMENSIONAL ELECTROPHORESIS (2D ELECTROPHORESIS) 2. Standard separation of proteins is done in one direction 3. This is followed by SDS-PAGE in perpendicular direction 4. This results in hundreds of identifiable protein peaks Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 10. 10 ISOELECTRIC FOCUSSING 1. Gives superior resolution to closely migrating proteins 2. Here the gel used contains a gradient of pH established by using ampholytes 3. As each protein reaches the gel location where the pH equals its own, the net charge becomes zero 4. It cannot move further 5. Thus proteins move here strictly on the basis of their pH Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 11. 11 * ANCILLARY TECHNIQUES PRECIPITATION 1. The sample to be tested usually contains a lot of undesired proteins. 2. These undesired proteins can be removed by precipitation so that a single minor protein can be isolated by electrophoresis. 3. First the value of total proteins is found out 4. Then Sodium sulfate, sodium sulfite, ammonium sulfate or methanol is used to precipitate globulins. 5. Protein estimation from the remaining solution after precipitation can give an idea about the albumin concentration – electrophoresis can give an idea about the types of proteins apart from globulins. 6. globulin = total protein – albumin 7. estimation of albumin : globulin ratio is useful in various disorders Normal : A:G ratio >1:5 (1-3) Decreased A:G ratio Decreased albumin Malnutrition Malabsorption Liver failure Proteinuria Accumulation of ascetic fluid Enteropathy Increased A:G ratio ************ Increased globulins Acute or chronic infections Myelomas Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 12. 12 COLUMN SEPARATION (1) Gel filteration: 1. Media such as agarose beads/sephadex is used 2. They have beads in them with pores of various sizes 3. Largest proteins cannot pass through pores in the beads – they pass through spaces in beads and are eluted first 4. Medium sized proteins pass through medium sized pores and appear second. 5. Small sized proteins pass through small sized pores and are eluted last. Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 13. 13 (2) Ion Exchange Chromatgraphy 1. This is of two types – Anion exchange and Cation exchange chromatography 2. This technique uses charged particles which are placed in the column. 3. When proteins having the opposite charge as the column pass through it, they are retained for a longer time, neutral elute the second while same charged particles elute first. ANION EXCHANGE CHROMATOGRAPHY 1. Media such as DEAE or QAE are used with have net positive charge. 2. Albumin, α and some β globulins which are anions stick to positively charged matrix. 3. γ globulins that have no charge are eluted faster. CATION EXCHANGE CHROMATOGRAPHY 1. Media such as carboxymethylcellulose are used which have a negative charge. 2. Positively charged cations stick to the matrix 3. Albumin is eluted first here Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 14. 14 (3) Hydrophobic chromatography 1. In this technique, support medium interacts with proteins according to their hydrophobic nature. 2. Here ‘high salts’ and ‘low salts’ are used 3. high salts structure water around themselves and expose the hydrophobic ends of proteins 4. these hydrophobic ends get attracted toward the medium and stick to it 5. according to hydrophobic nature of proteins, they stick or are eluted 6. ‘low salts’ are used to elute as they donot / expose less number of hydrophobic ends. Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 15. 15 (4) Affinity chromatography 1. This is based on specific binding between a protein of interest and another protein (can be its antibody/antigen) bound to the solid medium. 2. Bound protein can then be eluted in its purified form. 3. examples a. to separate FVII-vWF – column is incorporated with monoclonal antibody to vWF b. Igs can be separated by using Staphylococcal protein A in gel matrix c. Attaching dihydroxyboronate to medium helps separate glycosylated hemoglobin d. To separate digoxin – digibind is used CroFab – crotalid snake venom Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 16. 16 (5) Capillary electrophoresis 1. This procedure is similar to HPLC in that a column is employed where separation of molecules is done on the basis of size/hydrophobicity or strereospecificity. 2. Applicable to large molecules such as DNA. Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 17. 17 * SUMMARY OF WORK FLOW Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 18. 18 * APPLICATIONS (1) SERUM PROTEIN ELECTROPHORESIS Following patterns are observed in normal conditions and various disorders on electrophoresis. Normal: Cirrhosis of liver: When liver function is sufficiently diminished, protein synthesizing capacity is compromised and concentrations of albumin and proteins in the alpha and beta bands are decreased. An additional common finding is beta-gamma bridging due to increased IgA. Beta-gamma bridging Alb α1 α2 β γ Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 19. 19 The Nephrotic Syndrome -1. Renal disease involving the glomeruli is always associated with increased urinary protein loss. When protein loss is greater than 3-4 g/day, the protein synthesizing capacity of the liver is exceeded and hypoproteinemia, accompanied by anasarca, develops to cause the nephrotic syndrome. 2. The massive urine protein loss is due to increased permeability of glomeruli to protein. The permeability increase may be minimal so that only albumin and other smaller molecular weight proteins are selectively filtered (selective nephrosis, as in Minimal Change Disease) or may be greater so that larger proteins are also filtered (nonselective nephrosis, as in membranous golmerulonephritis) as is the case in the example shown. 3. Alpha-2-macroglobulin is sufficiently large so that it is not filtered and increased synthesis (from the general hepatic protein synthesis) causes its accumulation. 4. Lipoproteins are also sufficiently large to accumulate and hyperlipidemia is a characteristic of the nephrotic syndrome, although lipoproteins are not stained with the protein stain used in visualizing proteins. Normal Abnormal Alb α1 α2 β γ Alpha-1-Antitrypsin Deficiency: A genetic defect causes a deficiency of alpha-1-antitrypsin. The antiprotease deficiency results in a propensity to develop emphysema. Since alpha-1-antitrypsin is the major component of the alpha-1 band, deficiency is suggested by a reduced alpha-1 band. Deficiency is confirmed by specific immunochemical quantification. Normal Abnormal Alb α1 α2 β γ Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 20. 20 Acute Inflammation The alpha-1 and alpha-2 bands are increased during the inflammatory response from increased hepatic synthesis of acute phase reactant proteins. Normal Abnormal Alb α1 α2 β γ Chronic Inflammation -Immunoglobulin synthesis by antigen activated B lymphocytes transformed to plasma cells is demonstrated by the increased polyclonal gamma band. Normal Abnormal Alb α1 α2 β γ Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 21. 21 Immunoglobulin Deficiency -Deficient immunoglobulin synthesis is revealed by a markedly diminished gamma band. Effected individuals are prone to recurrent infection Monoclonal Gammopathy -1. An unusually sharp band in the gamma region strongly suggests the presence of a homogeneous immunoglobulin and, thus, the malignant proliferation of plasma cells from a single cell (multiple myeloma) in contrast to the broad, heterogeneous, or polyclonal, gamma band as exhibited above in chronic inflammation from immunoglobulin synthesis by many different clones of plasma cells. 2. Homogeneous immunoglobulins are also found in Waldenstrom's macroglobulinemia (where the sharp gamma band is always IgM). Specimens which exhibit a narrow gamma band are further examined by immunofixation electrophoresis as described below Alb α1 α2 β γ (2) CSF ELECTROPHORESIS Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 22. 22 1. The diagnosis of Multiple sclerosis is ultimately a clinical one based on neurologic history and physical examination. 2. Nevertheless, advanced laboratory results such as elevated IgG indices and presence of oligoclonal bands of IgG or Kappa /lambda light chains on CSF electrophoresis, as well as neuroimaging techniques have proven to be invaluable in diagnosis of MS. Agarose gel electrophoresis 1. Concentrated CSF is used as sample 2. Shows discrete bands of IgG – the oligoclonal bands 3. Presence of two or more bands is necessary for diagnosis 4. False positive results are obtained in SSPE, CNS infections like neurosyphilis, Crypotococcal meningitis, GBS, transverse myelitis, burkitt’s lymphoma etc. 5. Sensitivity is less than other methods of electrophoresis Staining Commassie brilliant blue/paragon violet/silver staining 1. silver staining is more sensitive then CBB 2. however these techniques must be simultaneously carried out on patients serum also because polyclonal gammopathy can lead to diffusion of immunoglobulin into CSF and lead to false positive results. This is seen in case of liver diseases, SLE, RA and chronic granulomatous diseases. ImmunoFixation Electrophoresis 1. Immunofixation electrophoresis (IFE) is used to demonstrate that a narrow gamma band is due to a homogeneous immunoglobulin. 2. In the illustration below, 6 replicates of the specimen are loaded on to separate lanes of an IFE gel. 3. Following electrophoresis, the protein in each lane is stained differently. 4. The first lane (SP) is stained for total protein. 5. The protein in each of the other lanes is "stained" with specific antisera for immunoglobulin heavy and light chains, respectively, as illustrated in the figure. 6. The finding of the preponderance of only one light chain associated with a predominantly staining heavy chain confirms the molecular homogeneity of the immunoglobulin and also provides identification. 7. IFE identifies the narrow band as monoclonal IgG, lambda. 8. Sometimes malignant plasma cells synthesize excess light chains and less frequently only light chains are synthesized. Almost never is excess heavy chain or only heavy chain synthesized. Excess free lambda light chain is exhibited in the illustration. Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 23. 23 a. Lymphocytic pleocytosis and 2 plasma cells in the CSF cytospin preparation. b. 4b. Isoelectric focusing/immunofixation revealed CSF-restricted oligoclonal IgG bands as well as identical paraprotein bands in CSF and serum. Anode is on the left. c. 4c. Serum immunofixation electrophoresis revealed the presence of IgGκ monoclonal band (arrow). Anode is at the top. ELP, electrophoresis (general protein stain); G, A, M, K, L: immunofixation for γ, α, μ, κ and λ chain, respectively. d. 4 d. Isoelectric focusing/affinity-mediated immunoblotting analysis: Paraprotein bands did not react with Borrelia antigen but partly obscured CSF-restricted oligoclonal IgG pattern. Paired CSF and serum samples tested for (from left to right) "total" IgG, IgGκ, IgGλ; Anti-Borrelia IgG, IgGκ, IgGλ. Anode is at the top. Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 24. 24 (3) URINE ELECTROPHORESIS 1. 2. 3. 4. 5. 6. 7. The main reason for performing urine protein electrophoresis is to find a light chain myeloma producing an excess of free light chains (Bence Jones protein), an important part of a myeloma screen. A band in the urine protein electropherogram may also result from an intact monoclonal immunoglobulin, especially if the patient has poor renal function. Immunofixation is important in defining the nature of the band and in distinguishing between Bence Jones protein and an intact monoclonal protein originating from the serum. From the urine electropherogram we can also tell if the proteinuria is of glomerular origin with a predominance of albumin, or if it has tubular components with excretion of smaller molecular weight proteins such as retinol binding protein and alpha-1 microglobulin. Fragmented albumin in urine is occasionally seen but is of unknown significance. Historically, urine has been concentrated by either removal of water from the specimen leaving the proteins in higher concentration, or by centrifugation whereby the proteins are spun away from the majority of the water. Demonstration of the protein components of urine from concentrated specimens was originally performed on cellulose acetate and later on agarose and high resolution agarose gel. Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics
- 25. 25 (4) HEMOGLOBIN ELECTROPHORESIS Rationale: 1. Haemoglobin (Hb) abnormalities are the most frequent genetic disease, affecting approximately 7 per cent of the world population. 2. Today, abnormal Hbs are generally discovered during a systematic study performed within programmes for prevention of thalassaemias or sickle cell disease. 3. In several regions (India, Turkey, Irak, Iran, Gaza strip, Saudi Arabia, Cyprus, etc.), these are found during a premarital screening. In other regions, like west Europeans countries, the research for the main Hb disorders is often limited to populations at risk. It is done either as preconceptional or neonatal screening programmes. Methods and patterns: 1. Hb S [β6 Glu>Val], the first abnormal Hb described, was discovered in 1949 by Pauling et al using moving boundary electrophoresis. 2. Zone electrophoresis performed on cellulose acetate strips (CAE) is still used in many clinical laboratories. 3. This technique has a resolution lower than that of IEF, but because of its simplicity remains among the more popular methods used in Hb screening. In this technique, the Hb molecules are separated at alkaline pH. Under these conditions all Hbs have a negative charge and migrate towards the cathode. Hb S, which has an additional positive charge compared to Hb A migrates more slowly. 4. In IEF, a pH gradient is established by carrier ampholytes submitted to an electric current and the Hb molecules migrate across this gradient until they reach the position where their net charge is zero (isoelectric point). The molecules will then concentrate in a sharp band as illustrated in Fig. 5. This technique allows separating molecules with isoelectric points differing only by 0.02 pH unit. Hb D-Punjab [β121 Glu>Gln], not detectable from Hb S by CAE, could easily be recognized by this technique. The disadvantage of this method is its relatively high cost and the requirement for a well-experienced laboratory staff. 6. This technique can help in diagnosing various hemoglobinopathies. Notes on electrophoresis.. By Dr. Ashish V. Jawarkar Contact: pathologybasics@gmail.com Facebook: facebook.com/pathologybasics