Sickle cell Anemia
•
19 j'aime•10,398 vues

This a series of notes on hematology useful for undergraduate and postgraduate medical and paramedical students. Notes are prepared from standard texts and are easy to reproduce in exams.

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (13)
Similaire à Sickle cell Anemia
Similaire à Sickle cell Anemia (20)
Plus de Ashish Jawarkar
Plus de Ashish Jawarkar (20)
Dernier
Dernier (20)
Sickle cell Anemia
- 1. 1 SICKLE CELL ANEMIA Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 2. 2 OVERVIEW 1. 2. 3. 4. 5. 6. 7. 8. 9. Pathology Types Distribution Pathogenesis Factors that influence sickling a. concentration of HbS b. Other types of Hb c. MCHC d. Oxygen tension e. Temperature f. Low pH Clinical features (sickle cell anemia) Lab diagnosis a. Red cell indices b. P.S. c. ESR d. Bone marrow e. Sickling test f. Hb electrophoresis g. Solubility test h. Neonatal screening i. Prenatal screening Principles of therapy Sickle cell trait Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 3. 3 * PATHOLOGY Caused by mutation in beta globin gene – at sixth position, glutamic acid is replaced by valine * TYPES 1. Sickle cell anemia Homozygous state for HbS (βs βs) >70% Hb is HbS 2. Sickle cell trait Heterozygous carrier state for HbS (βs β) 25-40% of Hb is Hbs 3. Sickle cell – β thalessemia Double heterozygote in which sickle cell gene is inherited from one parent and beta thal gene from other parent (βs β0) or (βs β+) 4. Combination of HbS with other abnormal hemoglobin (HbSD, HbSC, HbSO (arab disease), HbSE disease) * DISTRIBUTION 1. Prevalent in Africa, middle east and Central and south India 2. High prevalence in areas of high malaria endemicity Sickle cell is said to provide protection against P. falciparum – P. falciparum infested RBCs are rapidly phagocytosed and destroyed due to rapid sickling The theory of balanced polymorphism – Because sickle cell provides protection against malaria, sickle cell genes are preferentially selected over normal genes in endemic areas, giving a high prevalence of sickle cell patients. Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
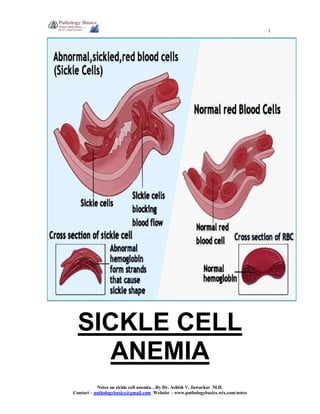
- 4. 4 * PATHOGENESIS Red cells with HbS Passage through microcirculation in spleen Low O2 tension Arrangement of fibres along the long axis of the red cell Delay time/ lag time Sickling of the cell on formation of a polymer of critical size – k/a nucleation phase Cells passing through tissues with good O2 tension Desickling Repeated cycles of sickling and desickling Irreversibly sickled red cell Lyse by themselves in Circulation macrophage phagocytosis in spleen Intravascular hemolysis vascular stasis adherence to endothelium extravascular hemolysis Platelet activn Chronic hemolytic anemia Autosplenectomy Spleen in hands and feet, head of femur And renal papillae Hyposplenism (decreased fn of spleen) Infection by capsulated org like pneumococcus Vasculr occlusion Damage and necrosis of various organs Dactylitis, necrosis of femoral head Renal papillary necrosis Typhoid Osteomyelitis Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 5. 5 * FACTORS THAT INFLUENCE SICKLING (i) INTRACELLULAR CONCENTRATION OF HbS Sickle cell trait patients have less concentration of HbS and so there is less tendency to sickle. Sickle Cell anemia patients on the other hand have greater tendency of their red cells to sickle (ii) OTHER TYPES OF Hb HbF does not participate in sickling Hence infants, heterozygotes for HbF and Hereditary persistence of fetal hemoglobin patients donot have significant sickling. (iii) MCHC Increased MCHC due to cellular dehydration favours increased contact between HbS strands and favours sickling. This factor is responsible for sickling in renal medulla (hyperosmolar mileu causes dehydration) (iv) OXYGEN TENSION HbSS cell sickle at PO2 – 40 mm Hg HbAS cell sickle at PO2 – 15 mm Hg (v) TEMPERATURE Cold induces vasoconstriction and may cause sickling episodes (vi) LOW Ph Acidosis increases sickling Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 6. 6 * CLINICAL FEATURES 1. 2. 3. 4. 5. 6. 7. 8. 9. Symptoms start around 3-4 months of age as the level of HbF falls Anemia of variable degree is present, more in sickle cell anemia, less in sickle cell trait Splenomegaly in infants and young children : due to RE system hyperplasia Splenectomy later in life : due to autoinfarction Increased risk of infection due to capsulated organism like s. pneumonia and H. influenzae – due to impairment of phagocytic function Salmonella osteomylitis Jaundice and hepatomegaly Signs of vasoocclusive events a. Recurrent leg ulcers b. Dactylitis c. Acute abdominal pain due to visceral infarcts d. Renal papillary necrosis e. Priapism f. Pulmonary infarction and acute chest syndrome g. Sickle retinopathy – salmon patches due to intra retinal hemorrhages h. Spontaneous abortions Crises in sickle cell anemia a. Sickling crises Pain in abdomen, bone pain, chest pain and stroke Precipitated by fever, dehydration and infections like malaria b. Hemolytic crises Sudden lowering of Hb Reticulocytosis Increased bilirubin (indirect) Sudden increase in rate of hemolysis c. Aplastic crises Due to infection with Parvovirus B19 Bone marrow shows giant proerythroblasts with intranuclear inclusions d. Sequestration crises Seen in sickle β thal or HbSC disease Massive sequestration of sickled red cells in spleen Decreased blood volume Shock Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 7. 7 * LABORATORY DIAGNOSIS 1. RBC Indices Hb – 6-9 gm/dL TLC on counter – elevated with lymphocytosis Actually count is falsely elevated due to normoblasts in peripheral blood Platelet count may be elevated – splenic trapping is lacking 2. Peripheral Smear a. moderate to severe anisopoikilocytosis b. Normocytic, normochromic anemia c. 5-10 % cells may be irreversibly sickled d. Polychromasia e. Few RBCs demonstrate Howell Jolly bodies 3. Retic count Reticulocytosis 3-10% 4. ESR Is low – because sickled cells fail to rouleaux 5. Bone marrow a. erythroid hyperplasia b. Normoblastic reaction c. Iron stores are increased d. Myelopoeisis and megakaryopoeisis are normal 6. Laboratory tests a. Sickling test Sickling can be demonstrated by use of a reducing agent like 2% sodium metabisulfite or sodium dithionite Principle Sodium metabisulphite reduces the oxygen tension inducing the typical sickle-shape of red blood cells. Sample Fresh blood in any anticoagulant. Reagents 0.2 g of sodium metabisulphite in 10 ml of distilled water. Stir until dissolved. Prepare fresh each time. Method 1. Mix 1 drop of blood with 1 drop of 2% sodium metabisulphite solution on a microscope slide. Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 8. 8 2. Cover with a cover slip and seal the edge with wax/vaseline mixture or with nail varnish. Allow to stand at room temperature for 1 to 4 hours. 3. Examine under a microscope with the dry objective. Interpretation In positive samples the typical sickle-shaped red blood cells will appear. Occasionally the preparation may need to stand for up to 24oC. In this case put the slides in a moist Petri dish. False negative results may be obtained if the metabilsulphite has deteriorated or if the cover slip is not sealed properly. A positive test does not distinguish the sickle cell trait from sickle cell disease. It is important to examine the preparation carefully and in particular near the edge of cover slip. adding Sodium metabisulfite Before after Limitations 1. does not differentiate between sickle cell anemia and sickle cell trait 2. cannot be used for mass screening (microscopy is needed) Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 9. 9 b. Hb electrophoresis (only diagnostic test) 1. Variant haemoglobins such as haemoglobin S often differ in surface charge from each other and from normal adult haemoglobin, haemoglobin A. They can thus be differentiated from each other by electrophoresis on a starch block or cellulose acetate paper. 2. This slide shows the results of haemoglobin electrophoresis of the blood from a normal adult, a patient with sickle cell anaemia (SS) and people with sickle cell trait (AS) and haemoglobin C trait (AC). Haemoglobin C is another variant haemoglobin which, like haemoglobin S, is fairly common in people originating in West Africa or the Caribbean. Sickle cell anemia HbS : 80-95 % HbF : 5-15% HbA2: Normal Sickle cell trait HbS : 60% HbA : 40% Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 10. 10 c. Solubility test (screening test) PRINCIPLE 1. Test is based on the solubility difference between Hb S and Hb A in concentrated phosphate buffer solution. Red blood cells under test are lysed by a powerful hemolytic agent and the released hemoglobin is then reduced by sodium dithionite in a concentrated phosphate buffer. 2. In the presence of Sodium Dithionite, Hb S precipitates causing turbidity of the reaction mixture. Under the same conditions, Hb A, as well as most other hemoglobins, are soluble. 3. When subjected to a centrifugal force the precipitated hemoglobin (Hb S) forms a red precipitate on top layer leaving the lower solution clear and colourless. The soluble hemoglobin (Hb A) gives a clear red lower solution with a grey precipitate on the top layer and most HbAS which contains both precipitated and soluble hemoglobin gives a red precipitate ring on top layer with a light red to pink colour lower solution. INTERPRETATION d. HPLC (high performance liquid chromatography) Result : Hemoglobin variant with retention time in S window Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 11. 11 7. Neonatal screening Done to identify babies at risk so that they donot develop complications Tests done: Citrate agar electrophoresis Will develop sickle cell anemia HbF HbS No HbA Will develop sickle cell trait HbF HbS HbA Normal HbF HbA 8. Prenatal screening If parents are sickle cell trait, Chorionic villous sampling can be done at 10-12 weeks to see for sickle cell mutations Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 12. 12 * PRINCIPLES OF THERAPY 1. Prevent crises a. Treat infections b. prevent exposure to cold, stress, hypoxia and dehydration 2. Treatment of vasoocclusive episodes a. analgesics b. keep warm c. fluid intake maintainence d. oxygenation e. partial exchange transfusion 3. Transfusion therapy a. PCV transfusion During aplastic crises Acute splenic sequestration b. Regular chronic transfusion Keep sickle cells to <40% Prevent cerebrovascular accidents c. Partial exchange transfusion Vasoocclusive episodes d. Folic acid e. Hydroxyurea Increases HbF, decreases crises episodes 4. To avoid complications a. Pneumococcal vaccine b. Avoid OC pills c. Avoid radiographic contrast media Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes
- 13. 13 * SICKLE CELL TRAIT 1. Asymptomatic heterozygous state (βs β0) 2. HbS – 25-40%, HbA 65-70% 3. Hb 11-13 gm/dL Clinical features 1. asymptomatic 2. vasoocclusive episodes may occur at high altitudes 3. Papillary necrosis may occur with proteinuria and hematuria Peripheral smear 1. normocytic normochromic confirmed on 1. solubility test 2. sickling test 3. Hb electrophoresis Treatment Survival is normal, no treatment required Notes on sickle cell anemia…By Dr. Ashish V. Jawarkar M.D. Contact – pathologybasics@gmail.com Website – www.pathologybasics.wix.com/notes