Upper airway obstruction
•Télécharger en tant que PPTX, PDF•
114 j'aime•51,366 vues

airway obstruction

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Upper airway obstruction
Similaire à Upper airway obstruction (20)
Dernier
Dernier (20)
Upper airway obstruction
- 2. Contents Background History Location of obstruction Signs and symptoms Causes of airway obstruction Fixed vs variable obstruction Investigation Management
- 3. Background
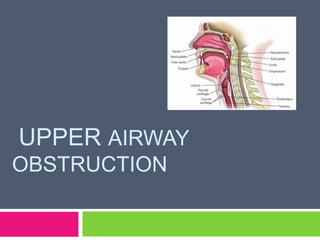
- 4. Upper airway includes Nose Nasopharynx Oropharynx Larynx (supraglottis, subglottis) Trachea (extrathoracic) Jacobson S. Upper airway obstruction. Emerg Med Clin North Am. 1989;7:205-17.
- 5. Upper airway is the segment of the conducting airways that extends between the nose (during nasopharyngeal breathing) or the mouth (during oropharyngeal breathing)and the main carina, located at the distal end of the trachea. Physiological points of narrowing are the nostrils, the velopharyngeal valve (at the passage between the nasopharynx and oropharynx), and the glottis Jacobson S. Upper airway obstruction. Emerg Med Clin North Am. 1989;7:205-17.
- 6. Common etiologies of upper airway obstruction in adults include infection, inflammatory disorders, trauma, and extrinsic compression related to pathology of adjacent structures. Definitive management depends on the underlying etiology and may include both medical and surgical interventions Jacobson S. Upper airway obstruction. Emerg Med Clin North Am. 1989;7:205-17.
- 8. In the mid-sixteenth century, the first successful tracheostomy was performed to relieve upper airway obstruction caused by a pharyngeal abscess. In the early nineteenth century, the procedure was used to treat croup, and diphtheria. By the turn of the twentieth century, rigid bronchoscopy was used to remove a foreign body from the trachea. Ikeda introduced the flexible bronchoscope in Jacobson S. Upper airway obstruction. Emerg Med Clin North Am. 1989;7:205-17. 1967.
- 9. Malignancy become more prevalent with increasing tobacco use and exposure to modern environmental toxins. Complications of endotracheal intubation and tracheostomy have become well recognized causes of benign upper airway stenosis. Jacobson S. Upper airway obstruction. Emerg Med Clin North Am. 1989;7:205-17.
- 10. Improvement in pharmacologic agents to treat infectious, inflammatory, and malignant etiologies, as well as developments in radiation oncology, have had significant effects on management of upper airway obstruction. Development of new endoscopic and imaging techniques and introduction of interventional pulmonology also have proved useful in the management of upper airway obstruction. Jacobson S. Upper airway obstruction. Emerg Med Clin North Am. 1989;7:205-17.
- 12. Upper Airway Obstruction Noisy Breathing Noise during INSPIRATION Noise during EXPIRATION Difficulty breathing IN Difficulty breathing OUT Proximal to Thoracic Inlet Distal to Thoracic Inlet Nose, pharynx, larynx Trachea, bronchi, peripheral airways Khosh MM, Lebovics RS. Upper airway obstruction. In: Parrillo JE, Dellinger RP, eds. Critical Care Medecine. St. Louis: . Mosby; 2001:808-25
- 13. Upper Airway Obstruction Difficulty breathing IN Awake/Crying IMPROVES Awake/Crying DETERIORATES Nose / Pharynx Larynx Khosh MM, Lebovics RS. Upper airway obstruction. In: Parrillo JE, Dellinger RP, eds. Critical Care Medecine. St. Louis: . Mosby; 2001:808-25
- 14. Where in the Airway is the Obstruction Snoring Naso pharynx Larynx Stridor Wheeze + + - + + Small babies Trachea & bronchi Small airways Severe obstructn + + + Khosh MM, Lebovics RS. Upper airway obstruction. In: Parrillo JE, Dellinger RP, eds. Critical Care Medecine. St. Louis:
- 15. Signs & Symptoms
- 16. The main symptoms of upper airway obstruction are dyspnea and noisy breathing. They are prominent during exercise and also may be aggravated by a change in body position. Breathing is labored in the recumbent position & may have a severely disrupted sleep pattern. Quan L. Diagnosis and treatment of croup. Am Fam Physician. 92419;6:747-55.
- 17. It also causes sleep apnea syndrome, which may resolve completely when the obstruction is relieved. Daytime somnolence may be a prominent feature of upper airway obstruction Quan L. Diagnosis and treatment of croup. Am Fam Physician. 92419;6:747-55.
- 18. In severely affected patients, cor pulmonale may occur as a result of chronic hypoxemia and hypercarbia. Typically, significant anatomic obstruction precedes overt symptoms. {for example, by the time exertional dyspnea occurs, the airway diameter is likely to be reduced to about 8 mm.} Quan L. Diagnosis and treatment of croup. Am Fam Physician. 92419;6:747-55.
- 19. Dyspnea at rest develops when the airway diameter reaches 5 mm, coinciding with the onset of stridor. Sound recordings from the neck and chest have shown that the sound signals from the asthmatic wheeze and stridor are of similar frequency. This explains why errors in diagnosis can be made and an upper airway obstruction due to a Quan L. Diagnosis and treatment of croup. Am Fam Physician. 92419;6:747-55. tumor or foreign body may be mistakenly treated
- 20. Neck flexion may change the intensity of stridor, suggesting a thoracic outlet obstruction. When the obstructing lesion is below the thoracic inlet, both inspiratory and expiratory stridor may be heard. Hoarseness may be a sign of a laryngeal abnormality. Muffling of the voice without hoarseness Quan L. Diagnosis and treatment a croup. Am Fam Physician. 92419;6:747-55. may represent of supra-glottic process.
- 21. Noise decreases as the severity of the obstruction increases so the complete absence of the sound is not the improvement in the symptoms but the complete blockage of tract. Quan L. Diagnosis and treatment of croup. Am Fam Physician. 92419;6:747-55.
- 22. Signs of hypoxemia are also present Anxiety Restlessness Tachycardia Pallor Cyanosis (late sign) Quan L. Diagnosis and treatment of croup. Am Fam Physician. 92419;6:747-55.
- 23. Causes of airway obstruction
- 24. Causes of obstruction can lies at any level of upper airway starting from nose till trachea. Cause includes can be of an infectious origin (bacterial, viral or fungal) or can be non infectious origin (tumours or foreign bodies) Khosh MM, Lebovics RS. Upper airway obstruction.In: Parrillo JE, Dellinger RP, eds. Critical Care Medecine. St. Louis: Mosby; 2001:808-25.
- 25. Nose “Blocked” nose (infants < 6 months) Choanal atresia Foreign body Polyps Allergy Khosh MM, Lebovics RS. Upper airway obstruction.In: Parrillo JE, Dellinger RP, eds. Critical Care Medecine. St. Louis: Mosby; 2001:808-25.
- 26. Oropharynx Main reason in this section of obstruction is adenoidal hypertrophy Foreign Nasal bodies polyp Tumors Khosh MM, Lebovics RS. Upper airway obstruction.In: Parrillo JE, Dellinger RP, eds. Critical Care Medecine. St. Louis: Mosby; 2001:808-25.
- 27. Larynx (supra glottis) Epiglotitis (bacterial or viral ) Laryngomalacia Congenital Vocal disorders like laryngeal web or cysts cords ( paralysis or papilloma) Khosh MM, Lebovics RS. Upper airway obstruction.In: Parrillo JE, Dellinger RP, eds. Critical Care Medecine. St. Louis: Mosby; 2001:808-25.
- 28. Larynx ( sub glottis) Main reason is this part is laryngo-tracheobronchitis (croup) Etiological Another agent is mainly Para influenza virus b reason is congenital sub glottic stenosis <6 months No history of infection Khosh MM, Lebovics RS. Upper airway obstruction.In: Parrillo JE, Dellinger RP, eds. Critical Care Medecine. St. Louis: Mosby; 2001:808-25.
- 29. Croup scoring system of Westley et al1 Croup score Symptoms 0 1 2 3 5 Stidor at rest None Audible with stethoscope Audible without stethoscope – – Retractions None Mild Moderate Severe – Air entry Normal Decreased Severely decreased – – Cyanosis None With agitation At rest – – Level of Normal – – – Altered consciousness Khosh MM, Lebovics RS. Upper airway obstruction.In: Parrillo JE, Dellinger RP, eds. Critical Care Medecine. St. Louis: Mosby; 2001:808-25.
- 30. Trachea Bacterial Foreign tracheitis body ingestion Retropharyngeal abscess Khosh MM, Lebovics RS. Upper airway obstruction.In: Parrillo JE, Dellinger RP, eds. Critical Care Medecine. St. Louis: Mosby; 2001:808-25.
- 31. Croup scoring system of Westley et al1 Croup score Symptoms 0 1 2 3 5 Stidor at rest None Audible with stethoscope Audible without stethoscope – – Retractions None Mild Moderate Severe – Air entry Normal Decreased Severely decreased – – Cyanosis None With agitation At rest – – Level of consciousness Normal – – – Altered
- 32. Angioedema Angioedema is characterized by welldemarcated swelling of the face, lips, tongue, and mucous membranes of the nose , mouth, and throat. When the larynx is involved, upper airway obstruction may occur and is fatal in as many as 25 % of patients. In most instances, the cause of angioedema is unclear; prior exposure to common allergens, such as drugs , chemical additives, and insect bites should be suspected. www.wikepedia.com/angioedema
- 33. They include reactions to histamine-releasing drugs, such as narcotics and radiocontrast materials, to aspirin and other nonsteroidal antiinflammatory drugs, and to angiotensinconverting enzyme inhibitors. Hereditary angioedema, a rare cause of upper airway obstruction, is an autosomal-dominant trait that occurs in all races. Hereditary angioedema is characterized by painless nonpitting edema of the face and upper www.wikepedia.com/angioedema airway
- 34. The underlying mechanism is a deficiency in production or function of C1 esterase inhibitor, a serum protease inhibitor that regulates the complement, fibrinolytic, and kinin pathways. Swelling progresses over many hours and then resolves spontaneously over 1 to 3 days. Death may occur from laryngeal obstruction. Emergency management includes securing the airway, administration of corticosteroids, and use of antihistamines and epinephrine. www.wikepedia.com/angioedema
- 36. Fixed obstruction Fixed obstructions of the upper airway are those whose cross-sectional area does not change in response to trans-mural pressure differences during inspiration or expiration. A fixed obstruction may occur in either the intrathoracic or extra-thoracic airways. Irrespective of the site of the obstruction, a fixed lesion results in the flattening of the flow-volume Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42 loop.
- 37. Non-distensible narrowing of the upper airway (fixed airway obstruction) occur in benign and malignancy strictures. Maximal inspiratory and expiratory flow-volume loops with fixed obstruction show constant flow, represented by a plateau during both inspiration and expiration. Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42
- 38. On the expiratory curve, the plateau effect is seen in the effort-dependent portion of the curve near TLC; very little change is noted in the effort-independent portion near residual volume. Since the inspiratory curve is similar in appearance, the ratio of FEF50% to FIF50% is normal (close to 1). The FIV1 and FEV1 are nearly the same in fixed upper airway obstruction. Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42
- 39. The flow-volume loop demonstrates a plateau of flow during inspiration and expiration, the FEF50%/FIF50% ratio is near 1. Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42
- 40. Variable extra thoracic obstruction A variable obstruction is one that eliciting varying degrees of obstruction during the respiratory cycle. Vocal cord paralysis is a common cause of variable extrathoracic obstruction. A variable extrathoracic airway obstruction increases the turbulence of inspiratory flow, and intraluminal pressure falls markedly below atmospheric pressure. This leads to partial collapse of an already narrowed airway and a Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42 plateau in the inspiratory flow loop.
- 41. Expiratory flow is not significantly affected, since the markedly positive pressure in the airway tends to decrease the obstruction. The ratio of FEF50% to FIF50% is high (usually > 2). Similarly, the FEV1 is > the FIV1. Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42
- 42. . Flow-volume loop shows inspiratory obstruction.FEF50%/ FIF50% is very high, and the inspiratory curve is flattened. Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42
- 43. Variable intra thoracic obstruction A variable obstruction in the intrathoracic airways show predominant reduction in maximal expiratory flow is associated with a relative preservation of maximal inspiratory flow. This association occurs because intrapleural pressure becomes markedly positive during forced expiration and causes dynamic compression of the intrathoracic airways. The obstruction caused by an intrathoracic lesion is accentuated and a plateau in expiratory flow occurs on the flow-volume loop. Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42
- 44. During inspiration, intrapleural pressure is markedly negative; therefore, the obstruction is decreased. The ratio of FEF50% to FIF50% is very low and may approach 0.3. The FEV1 is considerably < the FIV1. Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42
- 45. Although the flow ratios are similar to those seen in patients with COPD and chronic asthma, these disorders often can be distinguished by expiratory curve in patients with COPD and asthma is primarily altered in the effort-independent portion of the curve, leading to a characteristic shape unlike the plateau configuration of an upper airway obstruction Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42
- 46. Superimposed flow volume loops show a plateau of expiratory flow preceded by a peak of flow at higher lung volumes. The forced inspiratory flow is preserved in comparison to expiratory flow, but it is also reduced. FEF50%/FIF50% is 0.4 Steinert R, Lullwitz E. Failed intubation with case reports. HNO. 1987;35:439-42
- 47. Investigation
- 48. Quick history and physical examination :most important diagnostic tool in diagnosis of airway obstruction. In cases of severe acute upper airway obstruction (UAO) every single minute counts and doctors don’t have enough time for specific investigation before commencement of treatment. Goldberg J, Levy PS, Morkovin V, Goldberg JB. Mortality from traumatic injuries: a casecontrol study using data from the national hospital discharge survey. Med Care. 1983;21: 692-704.
- 49. It is useful to separate patients with potential UAO into those with severe symptoms and impending respiratory failure and those with a more indolent course and less severe symptoms. Airway resistance varies inversely with the fourth power of the radius at the point of UAO, and that small changes in the underlying Goldberg J, Levy PS, may dramatically worsen respiratory pathology Morkovin V, Goldberg JB. Mortality from traumatic injuries: a casecontrol study using data from the national hospital discharge survey. Med Care. 1983;21: 692-704. airflow.
- 50. Plain neck and chest radiographs Plain neck and chest films may be useful as screening tests by identifying tracheal deviation, extrinsic compression, or radiopaque foreign bodies. Lateral neck radiographs are considered insensitive and may result in unnecessary delay Goldberg J, Levy PS, Morkovin V, Goldberg JB. Mortality from traumatic injuries: a in securing the airway casecontrol study using data from the national hospital discharge survey. Med Care. 1983;21: 692-704.
- 51. Spirometry :- in gradual and mild cases of obstruction not in acute cases. CT scan :important investigation and in stable or in unstable pts with secured airway. High-resolution CT of neck and chest can help identify intrinsic and extrinsic tumors, vascular structures, and foreign bodies Goldberg J, Levy PS, Morkovin V, Goldberg JB. Mortality from traumatic injuries: a casecontrol study using data from the national hospital discharge survey. Med Care. 1983;21: 692-704.
- 52. Bronchoscopy : Rigid or flexible bronchoscopy with direct visualization is the most effective tool in establishing diagnosis and frequently provides the best way to correct UAO. Rigid bronchoscopy can be used in an emergency department to secure the airway. Flexible bronchoscopy can be used to establish the diagnosis as well deliver treatment including laser therapy, electrocautery, electrosurgery, balloon bronchoplasty, once the airway has been Goldberg J, Levy PS,and theGoldberg JB. Mortality from traumatic injuries: a secured Morkovin V, patient stabilized casecontrol study using data from the national hospital discharge survey. Med Care. 1983;21: 692-704.
- 53. Management
- 54. Establishing a secure and patent airway is the most important goal in the resuscitation of a patient with acute UAO. Quick history and clinical examination can help in determining the site of obstruction. In the outpatient setting the most common cause of UAO is obstruction of the larynx with a Goldberg J, Levy PS, Morkovin V, Goldberg JB. Mortality from traumatic injuries: a foreign body casecontrol study using data from the national hospital discharge survey. Med Care. 1983;21: 692-704.
- 55. Heimlich maneuver is recommended for relief of the airway obstruction in adults and children one to eight years of age subdiaphragmatic abdominal thrust can force air from the lungs; this may be sufficient to create an artificial cough and expel a foreign body from the airway. Goldberg J, Levy PS, Morkovin V, Goldberg JB. Mortality from traumatic injuries: a casecontrol study using data from the national hospital discharge survey. Med Care. 1983;21: 692-704.
- 56. Most important management is medical management which tried are Oropharyngeal airways Endotracheal intubation (transnasally or orally) Racemic epinephrine Corticosteroids Helium–oxygen mixture Goldberg J, Levy PS, Morkovin V, Goldberg JB. Mortality from traumatic injuries: a casecontrol study using data from the national hospital discharge survey. Med Care. 1983;21: 692-704.
- 57. Surgical intervention which forms the most important part of treatment in severe emergency Fiberoptic intubation Cricothyroidotomy Tracheostomy Laser/electrocautery/balloon dilation Airway stenting Goldberg J, Levy PS, Morkovin V, Goldberg JB. Mortality from traumatic injuries: a casecontrol study using data from the national hospital discharge survey. Med Care. 1983;21: 692-704.
- 58. Algorithm for UAO Goldberg J, Levy PS, Morkovin V, Goldberg JB. Mortality from traumatic injuries: a casecontrol study using data from the national hospital discharge survey. Med Care. 1983;21: 692-704.