How Cognitive Behavioral Model Explains Relapse
•
25 j'aime•11,426 vues

By Stephen Keeley, MS, CADC III, CGAC II, at May 2011 Oregon Problem Gambling Services Spring Training. Please contact presenters for use or sharing of presentation material.

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (18)
Similaire à How Cognitive Behavioral Model Explains Relapse
Similaire à How Cognitive Behavioral Model Explains Relapse (20)
Plus de Oregon Problem Gambling Services
Plus de Oregon Problem Gambling Services (20)
Dernier
Dernier (20)
How Cognitive Behavioral Model Explains Relapse
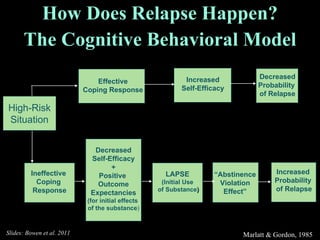
- 1. How Does Relapse Happen? The Cognitive Behavioral Model Marlatt & Gordon, 1985 High-Risk Situation Effective Coping Response Increased Self-Efficacy Decreased Probability of Relapse Ineffective Coping Response Decreased Self-Efficacy + Positive Outcome Expectancies (for initial effects of the substance ) LAPSE (Initial Use of Substance ) Increased Probability of Relapse “ Abstinence Violation Effect” Slides: Bowen et al. 2011
- 2. Relapse Prevention Therapy Marlatt & Gordon, 1985 High-Risk Situation Ineffective Coping Response Decreased Self-Efficacy + Positive Outcome Expectancies (for initial effects of the substance ) LAPSE (Initial Use of Substance ) “ Abstinence Violation Effect” Self Monitoring, Inventory of Situations Coping Skills Training Stress Management, Relaxation Education about Immediate vs Delayed Effects Contract to limit use, Reminder Card (what to do if you lapse) Cognitive Restructuring: Lapse is a mistake vs a failure Slides: Bowen et al. 2011
- 5. Enhancing Relapse Prevention with Mindfulness Slides: Bowen et al. 2011
- 10. Awareness: From “automatic pilot” to awareness and choice Triggers: Awareness of triggers, interrupting habitual reactions Acceptance: Change relationship to discomfort, decrease need to “fix” the present moment Intentions of MBRP Balance and Lifestyle: Supporting recovery and maintaining a mindfulness Slides: Bowen et al. 2011
- 11. Session 1: Automatic Pilot and Relapse Session 2: Awareness of Triggers and Craving Session 3: Mindfulness in Daily Life Session 4: Mindfulness in High-Risk Situations Session 5: Acceptance and Skillful Action Session 6: Seeing Thoughts as Thoughts Session 7: Self-Care and Lifestyle Balance Session 8: Social Support and Continuing Practice Awareness, Presence MBRP Session Themes Mindfulness and Relapse Bigger Picture: A Balanced Life Slides: Bowen et al. 2011
- 15. Stop Observe Breath “ SOBER” Breathing Space Expand Respond Slides: Bowen et al. 2011
- 16. Urge Surfing Riding the wave, rather than giving into the urge and being wiped out by it. Staying with the urge as it grows in intensity, riding it to its peak. using the breath to stay steady as it rises and crests, knowing it will subside. Trusting that without any action on your part, all the waves of desire, like waves on the ocean, arise and eventually fade away.
- 17. urge time Slides: Bowen et al. 2011
- 18. Awareness of Triggers Situation/ Trigger An argument with my girlfriend . What moods, feelings or emotions did you notice? Anxiety, hurt, anger What sensations did you experience? Tightness in chest, sweaty palms, heart beating fast, shaky all over What thoughts arose? “ I can’t do this.” “ I need a drink.” “ Forget it. I don’t care anymore” Slides: Bowen et al. 2011
- 19. Mindfulness and Substance Use Disorders: The Research Slides: Bowen et al. 2011
- 25. Time x group interaction: p= .02 Time 2 x group interaction: p= .01 Percentage Any AOD Use Results: Substance Use MBRP = 2.1 days of use TAU = 5.4 days of use Slides: Bowen et al. 2011
- 26. Comorbidity Worse substance use treatment outcomes (e.g., Hodgins, el Guebaly, & Armstrong, 1995; Witkiewitz & Villarroel, in press) Depression has particularly strong relationship with craving and relapse (Gordon et al., 2006; Zilberman et al., 2007; Curran et al., 2000 ; Levy, 2008) 40% (in the U.S.) with depressive/anxiety disorders have co-occurring substance use disorders (NCS; Kessler, Nelson, McGonagle, Liu, et al., 1996) Slides: Bowen et al. 2011
- 27. Results: Depression and Craving Substance Use Craving Depression MBRP (Witkiewitz & Bowen, 2010) Slides: Bowen et al. 2011
- 28. Results: Depression and Craving TAU MBRP Substance Use Slides: Bowen et al. 2011
- 32. Thank you! Slides: Bowen et al. 2011
Notes de l'éditeur
- Designed for use with individuals in aftercare Used as a stand-alone addictions treatment Treatment for addictive and non addictive disorders show support for efficacy, alone and combined with other techniques. A meta-analysis (Irvin, et al., 1999), reviews the use of RP across varying addictive behaviors, supporting RP as an effective treatment across substances.
- Designed for use with individuals in aftercare Used as a stand-alone addictions treatment Treatment for addictive and non addictive disorders show support for efficacy, alone and combined with other techniques. A meta-analysis (Irvin, et al., 1999), reviews the use of RP across varying addictive behaviors, supporting RP as an effective treatment across substances.
- MBRP is the first treatment to integrate core mindfulness practices with cognitive-behavioral skills for the prevention of relapse It is currently designed as an aftercare program , that follows the same structure as MBSR and MBCT Components include formal mindfulness practices such as the body scan, sitting meditation and yoga, as well as informal practices such as mindfulness of routine activities and using mindfulness in the midst of stressful situations. This is combined with cognitive-behavioral strategies for coping with triggers, high-risk situations, cravings and urges.
- More aware, nonjudgmental stance Increasing ability to experience emotion (e.g., depression) without “automatically” reacting, thereby altering conditioned response of drug craving to negative affect Further, the effect of MBRP on substance use appears to be in part explained by a decrease in craving. We also found an interesting relationship between treatment, craving and negative affect which I do not have time to discuss here, but will be presented as a poster……