Acute cardiopulmonary and metabolic responses to high intensity interval training

Results from the present study quantify the effects of altering either the intensity of the work or the recovery interval when performing interval sessions consisting of 60s of work and 60s of recovery for multiple repetitions. The information provided may aid those interested in designing interval training sessions by providing ranges of values that could be expected for individuals who possess moderate levels of cardiopulmonary fitness. Using a work intensity of 80% or 100% VGO2peak and a recovery intensity of 0% or 50% VGO2peak, subjects were able to exercise within the ACSM recommended range for exercise intensity. Based upon the data it would appear that a protocol such as the 80/0 may be appropriate for those individuals who are just beginning a program or have little experience with interval-type activity. By contrast, a 100/50 protocol could not be completed by all of the subjects and therefore may be too intense for some individuals.

Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Acute cardiopulmonary and metabolic responses to high intensity interval training
Similaire à Acute cardiopulmonary and metabolic responses to high intensity interval training (20)
Plus de Fernando Farias
Plus de Fernando Farias (10)
Dernier
Dernier (20)
Acute cardiopulmonary and metabolic responses to high intensity interval training
- 1. Journal of Strength and Conditioning Research Publish Ahead of Print DOI: 10.1519/JSC.0000000000001414 Revisions to Manuscript # R371415 TITLE: ACUTE CARDIOPULMONARY AND METABOLIC RESPONSES TO HIGH- INTENSITY INTERVAL TRAINING (HIIT) PROTOCOLS USING 60S OF WORK AND 60S RECOVERY Running Head: Acute Responses to Various HIIT protocols Laboratory: CSULB KIN Exercise Physiology Laboratory Authors: Ralph Rozenek, James W. Salassi III, Nicole M. Mier, John Fleming Department: Department of Kinesiology Institution: California State University Long Beach Address: 1250 Bellflower Blvd. Long Beach, California, USA, 90840 Funding: None Author Contact Information Corresponding Author: Ralph Rozenek, Ph.D. Email: rrozenek@csulb.edu Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 2. Phone: 1-562-985-4083 Fax: (562) 985-8067 Abstract Low-volume, high-intensity interval training (HIIT) consisting of 60s work and 60s recovery (60s/60s) repeated for 10 repetitions has previously been found to produce beneficial cardiopulmonary, cellular, and metabolic adaptations in healthy and at-risk populations. There is currently relatively little information pertaining to the acute changes that take place during individual training sessions. The purpose of this study was to examine the acute physiological responses to 60s/60s x 10 HIIT protocols using several combinations of work and recovery intensities. Eleven healthy adults (mean age + s.d. = 26.0 ± 5.3 yrs) performed four HIIT trials on separate days at varying percentages of peak power output (PPO) that consisted of the following work/recovery intensities: a) 80% PPO/0% PPO (80/0); b) 80% PPO/50% PPO (80/50); c) 100% PPO/0% PPO (100/0) and; d) 100% PPO/50% PPO (100/50). 100/50 produced higher (p < 0.05) peak, average, and nadir %VGO2peak compared to the other protocols. Other than the nadir values resulting from the 80/0 trial, all trials produced average, peak, and nadir %VGO2peak and %HRpeak values that were within exercise intensity ranges (≈45-90% VGO2max; ≈65-90% HRmax) recommended by the American College of Sports Medicine (ACSM) for improvement of cardiopulmonary function. 80/50 and 100/0 produced similar average HR and peak HR, RPE, blood lactate and %VGO2peak values. However, the average %VGO2peak was significantly higher (~9.3% absolute) in 80/50. It appeared that use of the 80/0, 80/50, and 100/0 protocols would Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 3. be appropriate for individuals who are at the low to moderate end of the cardiopulmonary fitness spectrum. Keywords: Intermittent Exercise, Oxygen Uptake, Power Output, Blood Lactate, Rating of Perceived Exertion INTRODUCTION Low-volume high-intensity interval training (HIIT) has become an increasingly popular form of training for both athletic (3,27) and clinical populations (20,22, 26). Individual training sessions are comprised of scheduled repetitive periods of relatively high intensity work followed by recovery periods consisting of lower intensity work or rest. Programs can be tailored to emphasize either anaerobic or aerobic metabolic pathways or a combination of the two depending upon how the various training variables are manipulated. Variables include the durations and intensities of the work and recovery intervals, as well as the total number of intervals to be completed. Two long-known advantages of using interval-type training over continuous training have been that individuals can work at higher intensities than typically encountered during continuous training and more total work can potentially be performed (14,30). Regardless of the type of program, studies have shown HIIT to be effective and can produce beneficial cardiopulmonary and metabolic adaptations equal to or greater than those achieved with moderate intensity continuous training with considerably less time involvement (11,19). Since there are many ways the duration and intensity of an interval program can be controlled, it has been a challenge to find an optimized HIIT program (4,27). Further Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 4. complicating matters are how such factors as level of training, health status, age, and gender influence an individual’s reaction to interval training (4,24,43). Programs incorporating low volume, short duration work intervals (< 30s duration) performed at intensities described as “all out” (11,19, 21) or “supramaximal” (28,40) have been found to produce significant central and peripheral adaptations within a relatively short time period. However these types of programs may not be suitable for all individuals because of the high training intensities involved (44). As a consequence, Gibala et al. (20) have suggested using an interval protocol consisting of 60s of work and 60s of recovery (60s/60s) repeated for 10 repetitions. A rationale for this type of program has been that by using somewhat longer duration work intervals than those employed in all-out or supramaximal studies, relative work intensities could be reduced, thus accommodating HIIT to a wider range of individual capabilities. Several training studies incorporating this 60s/60s protocol have found significant beneficial cardiopulmonary, cellular, and metabolic adaptations in healthy individuals (25) as well as in those with coronary artery disease (13) and type II diabetes (29). From a practical perspective, a 60s/60s program appears to be time-efficient and well-tolerated even in populations where higher intensity training has not been traditionally used to a large degree (25,29). Although the 60s/60s x 10 repetition HIIT program appears to be effective, there is relatively little information pertaining to the physiological responses during individual training sessions. Work and recovery intensity combinations that would make the overall effect of a training session too intense may be ineffective because, in some cases, individuals may not be able to complete all prescribed intervals which would lead to a reduction in total training Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 5. volume and/or possibly limit participation in such a program (35). On the other hand, there may be combinations that can be completed but are not intense enough to produce the desired adaptations because thresholds for training intensity, duration, and/or volume have not been met. Since short-term responses will ultimately dictate the type and magnitude of training adaptations, it would be beneficial to identify the acute cardiopulmonary and metabolic responses to different types of HIIT training. Therefore the purpose of this study was twofold: 1) to characterize the acute responses of a 1:1 HIIT protocol consisting of 60s of work and 60s of recovery and; 2) to compare the acute responses for several combinations of work and recovery intensities when using this protocol with apparently healthy individuals. It was hypothesized that the 60s/60s x 10 interval training protocols incorporating the 100% PPO work interval intensities would produce the highest observed average, peak, and nadir cardiopulmonary and metabolic responses. METHODS Experimental Approach to the Problem Previous studies investigating 60s/60s x 10 repetition interval programs have primarily focused on training effects (13,25,29) with only limited information provided regarding acute responses to this type of activity (29). Although the studies generally found improvements in cardiopulmonary and metabolic function, they used various methods to determine work and recovery intensities for the training sessions. As an example, Hood et al. (25) had their subjects perform the work intervals at 60% of peak power output (PPO) with recovery intervals performed at 30 watts. By contrast subjects in the study by Currie et al. (13) performed the Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 6. work intervals at 89% PPO while recovery intervals were performed at 10% PPO. It would be expected that the subjects would respond differently to the individual training sessions and thus ultimately produce different training outcomes. From a practical point of view, the observed inconsistencies in the application of the work and recovery intensities would make comparison of results among the studies difficult. How individuals may respond to various combinations of work and recovery intensities is currently poorly characterized. For individuals who are interested in designing interval-type programs based upon a 60s/60s x 10 repetition format, it would be beneficial to know the time-course of the response as well as ranges of expected values for typical physiological measurements of interest. This study attempted to quantify and compare the acute physiological responses to a 60s/60s x 10 repetition format by controlling the work and recovery intensities using four different combinations of the two variables. The independent variable in this study was the work/recovery intensity combination used in each trial. Oxygen uptake, heart rate, rating of perceived exertion, and blood lactate concentrations were selected as the dependent variables because they are commonly used indicators of cardiopulmonary function and physiological stress. Work and recovery intensities were quantified as percentages of peak power output (PPO). The selected work intensities used during the work interval were selected because they represented intensities within an effort range generally considered moderate to heavy. The recovery interval intensities were chosen because they span the low to moderate range of exercise intensities and it is approximately within this range that lactate removal rates tend to be at their highest (2). By using the selected work and recovery intensities, it was thought that Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 7. this approach could be used to more clearly delineate the acute responses to a 60s/60s x 10 repetition interval training program. Subjects Eleven healthy, recreationally active adults (5 male, 6 females) ranging in age from 20 to 36 years (mean age + s.d. = 26.0 ± 5.3 yrs.) participated in the study. None of the subjects had participated in a regular high-intensity interval training program for at least 3 months prior to the start of the study. All subjects read and signed informed consent documents prior to participation and all protocols were approved by a university institutional review board for the protection of human subjects prior to the initiation of the study. Physical characteristics of all subjects can be seen in Table 1. [Insert Table 1 about here] Procedures Height, body mass, and body composition were determined using a stadiometer and a Bod Pod (LMI, Concord, CA, USA) calibrated to manufacturer specifications before testing each subject. An initial graded exercise test (GXT) was performed on a Lode Corival electronic cycle ergometer (Lode BV, Groningen, The Netherlands) to determine peak oxygen uptake (VGO2peak), peak heart rate (HRpeak), peak power output (PPO), and peak blood lactate concentrations [bLa]. The GXT began with an initial 5-minute warm-up period at 25 watts (W). Subjects were Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 8. encouraged to find a self-selected cadence to use throughout the test, typically between 70-90 revolutions x min-1 . The ergometer was capable of maintaining a constant prescribed power output when subjects pedaled at cadences between 50 and 120 revolutions x min-1 . Following warm-up, subjects rode at increasing power outputs with increments of 25 W x min-1 . Once 250 W for males and 150 W for females were reached, power output was then incremented by 10 W x min-1 until test termination. Criteria for test termination included: a plateau in VGO2, a drop in cadence below 50 rev x min-1 , signs and symptoms of exercise intolerance, or the subject decided to stop. The highest VGO2 value obtained meeting the test criteria was termed VGO2peak. A 5-minute active cool-down at 25 W was used during the recovery period. No signs or symptoms of exercise intolerance were observed during or following testing. Heart rate (HR) was monitored continuously with a Polar (Polar Electro, Oy, Finland) transmitter belt worn around the chest that was capable of sending data to a metabolic measurement system (Vacumed, Ventura, CA) used to measure gas exchange and ventilation for VGO2 determination. The highest HR value obtained meeting the test criteria was termed HRpeak. The standard error of measurement for repeated determination of HR expressed as a percentage (%SEM) was 4.1%. The gas analyzers were calibrated prior to every test using known gas concentrations (16% O2/4% CO2) and ambient air. A 3-liter syringe was used to calibrate the turbine flow meter. The %SEM for repeated VGO2 measurement s was 3.3%. Blood lactate concentrations were measured using a finger stick method (41). Samples were obtained at rest and immediately following the GXT. A Lactate Plus portable lactate analyzer (Nova Biomedical, Waltham, MA, USA) calibrated using low and high controls prior to each GXT and interval trial was used for the measurements. The %SEM for blood lactate concentration measurements Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 9. was 4.0%. Ratings of perceived exertion (RPE) were measured each minute during the GXT using the Borg 6-20 scale (8). The PPO obtained at VGO2peak was used to determine the relative work and recovery intensities implemented in subsequent HIIT trials. Four HIIT trials were conducted at varying percentages of PPO and consisted of the following work/recovery intensities: a) 80% PPO/0% PPO (80/0); b) 80% PPO/50% PPO (80/50); c) 100% PPO/0% PPO (100/0) and; d) 100% PPO/50% PPO (100/50). Each HIIT trial used a 1:1 work to recovery ratio and consisted of alternating 60s periods of work and recovery. This work/recovery cycle was repeated 10 times for a total duration of 20 minutes. Each 20-minute trial was preceded by a 5-minute warm-up period performed at 25 W and followed by a 5- minute recovery period at 25 W. During the 0% PPO phase of the 80/0 and 100/0 trials, resistance on the ergometer was reduced to 0W on the display (7W actual) while subjects actively maintained the pedal cadence from the previous work interval. Oxygen uptake and HR were recorded every 20s using the previously described methods. Blood lactate concentrations were measured at rest just prior to the start of warm-up period, at the end of the fifth work interval, and immediately following the last work interval. Ratings of perceived exertion were recorded at the end of each minute of work and recovery. During all phases of testing, subjects were requested to maintain their normal diets and hydration status. In addition subjects were to refrain from consuming caffeinated beverages and/or exercising at least four hours prior to the testing sessions. The four trials were performed in random order on different days at approximately the same time of day with each trial separated by at least 48 hours. Statistical Analyses Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 10. An a priori calculation of sample size using Minitab version 15 (Minitab, Inc. State College, PA) determined that a minimum of 10 subjects was sufficient to detect an absolute difference of 10.0% between trials with 80% power, α = 0.05, and an assumed standard deviation of 5.0% on the primary outcome measure of %VGO2peak. Collected data were initially analyzed using a repeated measures analysis of variance with trial and sex used as between subject factors and time as a within subject factor. When significance was observed, a single factor repeated-measures ANOVA was used for further analyses with a Tukey post-hoc follow- up. A Bonferroni correction for multiple comparisons was used where appropriate. Effect sizes for the main effect of trial were reported as eta2 (η2 ) with values of 0.01, 0.06, and 0.14 representing “small,” “medium, “ and “large” effects respectively, as suggested by Cohen (12). The Statistical Package for Social Sciences version 20 (SPSS Statistics, SPSS, Chicago, IL) was used for all analyses. Statistical significance was set at (p ≤ 0.05). RESULTS As expected males, on average, were taller, weighed more, and had lower body fat percentages than females (p < 0.05). Additionally the males produced higher values for VGO2peak and PPO than the females during the GXT (p < 0.05). However, no significant differences in the response to the intervals were observed between males and females, nor were any significant interactions (trial x time x sex) noted for any of the variables investigated (p > 0.05); hence data were pooled for the remaining analyses. It should be noted that only 7 of the 11 subjects completed all test trials. Four of the subjects were not able to complete the 100/50 trial. One Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
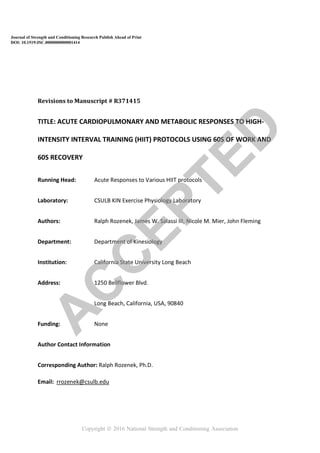
- 11. subject stopped as early as the fifth work interval, whereas the others completed at least 7 work intervals before stopping exercise. The response of VGO2 to the various interval trials is shown in Figure 1. Average, peak, and nadir, VGO2 values can be found in Table 2. A single-factor repeated-measures ANOVA showed a main effect of trial on the averaged %VGO2peak across intervals (F(3,30) = 98.39, p < 0.001, η2 = 0.669). Post-hoc analyses indicated that all four trials were different (p<0.05) from one another. The 100/50 trial produced the highest average %VGO2peak with a value of 82.8 + 6.2%, while the 80/0 trial produced the lowest value, 54.8 + 2.0%. A main effect of trial was observed for the peak %VGO2peak (F(3,30) = 38.23, p < 0.001, η2 = 0.547). The peak value for %VGO2peak, was highest while performing the 100/50 trial reaching 90.2 + 8.6% and was different (p < 0.05) from the other trials. The 80/0 trial elicited the lowest peak %VGO2peak value (67.5 + 6.3%) and was lower (p < 0.05) than all other trials. The 80/50 and 100/0 trials produced similar peak %VGO2peak values, 79.8 + 8.8% and 80.9 + 8.7% respectively (p > 0.05). However, both trials were different (p < 0.05) from either the 100/50 or 80/0 trials. In all trials the average and peak %VGO2peak values increased as the number of intervals increased up to completion of the fifth interval. With the exception of the 80/50 trial (p = 0.044), %VGO2peak did not increase beyond the fifth interval (p > 0.05). A main effect of trial for the nadir %VGO2peak values was also observed, F(3,30) = 195.60, p < 0.001), η2 = 0.763. The 100/50 trial produced the highest nadir value (%VGO2peak = 78.9 + 7.3%) while the lowest value resulted from the 80/0 trial (%VGO2peak = 43.6 + 7.5%). The 80/50 and 100/0 trials produced nadir %VGO2peak values of 72.6 + 8.9% and 51.7 + 9.9% respectively. Post- hoc analyses revealed that values for all trials were different from each other (p < 0.05). Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 12. With regard to the nadir %VGO2peak values, no differences (p > 0.05) were found from the first through the last interval in the 80/0 trial. Nadir %VGO2peak values were higher (p < 0.05) following the 5th interval compared to the first interval in the 80/50, 100/0, and 100/50 trials with no differences (p > 0.05) found beyond that point. [Insert Figure 1 about here] Heart rate responses expressed as %HRpeak can be seen in Figure 2. A main effect of trial on the average heart rate response (average %HRpeak) was observed (F(3,30) = 263.31, p < 0.001, η2 = 0.477). The 80/0 trial produced an average %HRpeak of 74.9 + 7.1% and was lower (p<0.05) than the other trials. By contrast, the 100/50 trial produced the highest average %HRpeak with a mean value of 90.9 + 3.8% which was higher (p < 0.05) than the others. There was no difference (p > 0.05) between the average %HRpeak values obtained from 80/50 and 100/0 trials (Table 3). The main effect of trial on Peak %HRpeak responses (F(3,30) = 32.88, p < 0.001, η2 = 0.403) showed a similar pattern to the average %HRpeak. The peak %HRpeak for the 80/0 and 100/50 trials were different (p < 0.05) than either the 80/50 or 100/0 trials with values of 83.2 + 5.5% and 94.6 + 3.0% respectively. The %HRpeak values of 88.8 + 5.9% for the 80/50 and 90.0 + 5.5% for the 100/0 trial were not different (p > 0.05) from one another. The main effect of trial also influenced the nadir % HRpeak values (F(3,30) = 72.78, p < 0.001, η2 = 0. 518). However, a somewhat different pattern of responses was observed with the average nadir HR responses. The nadir %HRpeak values of 67.8 + 10.2% for the 80/0 trial and 77.5 + 9.9% for the 100/0 trial were different (p < 0.05) than all other trials. The highest nadir %HRpeak value of 89.8 + 5.2 was Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 13. obtained during the 100/50 trial and was different than (p = 0.054) the nadir value of 85.3 + 7.2% obtained during the 80/50 trial. The number of intervals completed within a trial produced significant differences among the first, fifth, and tenth intervals (p < 0.05). As the number of intervals completed progressed, steady increases in the peak %HRpeak values were observed. By the end of the last interval in the 100/50 trials, peak HR values of 100.2 + 3.0% HRpeak were achieved. Nadir %HRpeak values also increased (p < 0.05) from the first through the tenth interval within each of the trials. However in the cases of the 100/0 and 100/50 trials no differences (p > 0.05) were observed for nadir %HRpeak between the fifth and tenth interval. [Insert Figure 2 about here] No difference in [bLA] was observed among the trials under resting conditions (F(4,50) = 0.598, p = 0. 666, η2 = 0.046) (Figure 3, Table 4). However [bLA] rose from rest to the end of the fifth work interval during each of the trials (p < 0.05). Significant differences were observed among groups at the end of the fifth (F(3,40) = 10.20, p = 0.001, η2 = 0.433) and also at the end of the final work interval (F(4,47) = 8.41, p < 0.001, η2 = 0.417). By the end of the fifth work interval, mean [bLA] during the 100/50 trial was higher (10.5 + 3.0 mmol x l-1 ) (p < 0.05) than either the 80/0 (4.9 + 1.9 mmol x l-1 ) or the 80/50 (6.8 + 2.6 mmol x l-1 ) trial, but not considered different (p > 0.05) from the 100/0 trial (8.5 + 2.3 mmol x l-1 ). Blood lactate concentrations at the end of the last work interval for the 80/0 trial were lower (5.0 + 2.4 mmol x l-1 )(p < 0.05) than the others (7.4 + 2.8 mmol x l-1 , 9.6 + 4.0 mmol x l-1 , and 10.2 + 2.7 mmol x l-1 for 80/50, 100/0, and 100/50 respectively) with no differences (p > 0.05) observed among the other trials. Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 14. Additionally [bLa] for the 100/0 and 100/50 trials at the end of the final interval were not different (p > 0.05) than the peak values obtained from the GXT (Table 1). No differences (p > 0.05) in [bLa] were noted between the end of fifth and final intervals within any of the trials. [Insert Figure 3 about here] A main effect of trial on the reported average RPE was observed (F(3,30) = 24.79, p = 0.001, η2 = 0.448) (Figure 4, Table 5). The average RPE for 80/0 trial (10.5 + 1.3) was lower (p < 0.05) than all other trials. By contrast average RPE for 100/50 trial (14.3 + 1.8) was higher (p < 0.05) than the 100/0 trial (12.5 + 1.7) but not the 80/50 trial (13.4 + 1.7) (p > 0.05). Differences in the peak RPE responses were also found (F(3,30) = 21.70, p = 0.001, η2 = 0.451). When averaged across an entire 20 minute interval session, peak RPE was lower (p < 0.05) in the 80/0 trial (12.6 + 1.1) compared to all others. The 100/50 trial (15.7 + 1.2) produced an average peak RPE response that was higher (p < 0.05) than all other trials. Similar peak RPE was observed in the 80/50 (14.3 + 1.5) and 100/0 (14.9 + 1.4) trials (p > 0.05). Differences were observed among the trials in the average nadir RPE response ((F(3,30) = 21.23, p = 0.001, η2 = 0.413). The 80/0 trial produced the lowest average nadir RPE with a value of 8.4 + 1.9. This was lower (p < 0.05) than either the 80/50 (12.4 + 2.2) or 100/50 (12.8 + 2.5) trial but not the 100/0 trial (10.0 + 2.3) (p > 0.05). Within each trial, Peak RPE increased significantly (p < 0.05) from the first to the fifth interval. However no significant differences were observed from the fifth interval onward in any of the trials. With the exception of the 80/50 trial where nadir RPE values increased (p < 0.05) from the first to the tenth interval, no Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 15. significant changes (p > 0.05) occurred as a result of increasing interval number in any of the other trials. [Insert Figure 4 about here] DISCUSSION Results of this study characterize the acute effects of varying either the work or recovery intensity during a 60s/60s interval program when intensity was based upon a percentage of PPO. Manipulating either the work or recovery intensity affected the overall response to an individual exercise session as exhibited by the significant differences of the average %VGO2peak response among the four interval trials. Other than the nadir values resulting from the 80/0 trial, all trials produced average, peak, and nadir %VGO2peak and %HRpeak values that were within exercise intensity ranges (≈45-90% VGO2max; ≈65-90% HRmax) currently recommended by the American College of Sports Medicine (ACSM) for the improvement of cardiopulmonary function (18). Altering the intensity of the recovery interval had a greater effect on the average %VGO2peak than changing the intensity of the work interval. For example, increasing recovery intensity from 0% PPO to 50% PPO resulted in a 19.8 + 4.7% absolute increase in the average %VGO2peak when performing at 80% PPO and a 17.4 + 7.0% increase during the 100% PPO trial. By contrast, increasing work interval intensity from 80% PPO to 100% PPO increased the average Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 16. %VGO2peak by an absolute amount of 10.6 + 6.5% when 0% PPO was used during recovery and only 8.1 + 5.0% when 50% PPO was used. Although the work interval intensity was lower, the 80/50 trial produced a significantly higher average %VGO2peak when compared to the 100/0 trial, whereas peak values were very similar. The addition of an active recovery period resulted in a smaller difference between the peak and nadir responses thus reducing amplitude, defined as the ratio of the difference between the work and recovery intensities divided by the average intensity (5), yielding higher overall average VGO2 and HR responses. From a metabolic standpoint, increasing the intensity of work during the recovery period would reduce the rate of phosphocreatine resynthesis (38,45), as well as alter blood lactate removal rates (31), the recharging of myoglobin stores (16), and the restoration of pH (15). These changes could potentially contribute to alterations to the oxygen uptake kinetics of subsequent work intervals (32) and thus affect the overall exercise response. Subjects had relatively little difficulty completing the 80/0 trial as demonstrated by the relatively low peak and average RPE responses as well as [bLa] which remained at approximately 5.0 mmol x l-1 from the end of the fifth work interval until completion of the session. On the other hand, The 100/50 trial was the only one where all ten of the prescribed intervals were not completed by all subjects. Only seven of the original eleven subjects were able to complete the 100/50 trial indicating that this trial was likely too intense for some subjects. Blood lactate concentrations were quite high, averaging above 10 mmol x l-1 from the end of the fifth work interval onward and were not significantly different than those observed at the end of the initial GXT. The leveling off of [bLa] during intermittent exercise has been reported previously (36,39) and thought to be a result of better balance between lactate Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 17. production and utilization as activity proceeds. The 100/0 trial resulted in [bLa] that was only slightly lower than the 100/50 trial, yet all subjects were able to complete it. This would suggest that elevated [bLa] may not have been responsible for fatigue in those who could not complete the 100/50 trial. In a previous study, Brickley et al. (9) found a significant correlation (r = 0.779; p < 0.05) between VGO2max and time to exhaustion at critical power. However in the current study it did not appear that a subject’s level of cardiopulmonary fitness, as determined by VGO2peak, had an effect on the number of intervals completed (r = 0.256; p > 0.05). Other factors potentially contributing to the onset of fatigue may have included those associated with central nervous system and/or metabolic function (1,17). The results suggest that using a recovery intensity of 50% PPO in combination with a work interval intensity of 100% PPO may be approaching the upper limits of what may be achievable in order to complete a 60s/60s x 10 repetition protocol for individuals who possess moderate levels of cardiopulmonary fitness. Contrary to the original hypothesis, the interval training sessions using the highest work intensities did not necessarily produce the largest average, peak, or nadir responses in the measured variables. In two of the trials, 80/50 and 100/0, average and Peak HR, RPE, [bLa], and peak %VGO2peak were all similar. However, the average %VGO2peak were significantly higher (~9.3% absolute) in the 80/50 trial. Although there were similarities in the two trials, it is possible that the observed subtle differences in responses to the 80/50 and 100/0 trials could ultimately produce different long-term adaptations. Both interval trials resulted in increased contribution of aerobic and anaerobic metabolism to overall energy demand during the activity. A potential benefit of utilizing the 80/50 or 100/0 formats as part of a regular training program may be that they would allow an individual to work at a relatively high percentage of VGO2peak while also Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 18. maintaining high [bLa] and completing the prescribed number of intervals. Repeated exposure to high lactate concentrations may stimulate adaptations leading to enhanced lactate removal (10), improved buffering capacity (19,42) and increased mitochondrial enzyme content (23) that could potentially improve an individual’s ability to tolerate high intensity exercise. Ideally when planning an interval training session, it should be designed in such a way as to meet a threshold for training intensity and allow for completion of the session so that sufficient duration and volume has also been attained (35). It has been stated (34) that highly trained individuals may need to exercise at intensities as high as 95-100% VGO2max to improve VGO2max, while for those who are moderately trained, exercise intensities in the range of approximately 70-80% VGO2max may be sufficient to produce aerobic adaptations. Furthermore, it has been suggested that the time spent training at PPO or the velocity associated with VGO2max may be an effective way to elicit improvements in performance (28,37). Billat et al. (6,7) have attempted to develop interval programs that allow individuals to operate at relatively high percentages of VGO2max for longer amounts of time when compared to endurance activity of similar intensity. In a relatively short duration interval protocol such as the one used in this study, only the 100/50 trial produced values that at their peak were just above 90% VGO2peak. The actual amount of time spent at this intensity would be rather low due to the fluctuations in VGO2 resulting from repeated transitions from exercise to recovery. If the amount of training time above 90% is important for athletic performance (33), then the 60s/60s protocol used in this study may not be optimal since the total training time was only 20 minutes and the highest average %VGO2peak and peak %VGO2peak observed during the 100/50 trial were 82.8 + 6.2% and 90.2 + 6.6% respectively. Although not measured in this study, it may be possible that the Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 19. individual average VGO2 responses were above lactate threshold or critical power and it is this effect repeated over a number of training sessions that eventually leads to adaptations rather than the short periods of time spent at PPO. Since interval exercise is sinusoidal in nature with the amplitude and frequency of the intervals being affected by the intensity and duration of the work and recovery intervals as well as the total number of intervals completed, attention should be given to both peak responses and the average response when considering long-term adaptations. Previous training studies using the 60s/60s protocol (13,25,29) have used work intensities ranging from 60% PPO up to 95% PPO. In the studies by Currie et al (13) and Little et al. (29) work rates during the intervals were individualized in order to obtain heart rates of approximately 73 + 10% of age-predicted maximum and 90% of maximum respectively. Recovery intensities in the various studies were at 10% PPO (13), 30W (25), or a choice between rest and 50W (29). Inconsistencies in the reporting of absolute and relative work rates or exercise intensity derived from either predicted or measured heart rates along with differences in recovery intensities have made it difficult to compare responses to these interval protocols. Despite the differences, beneficial adaptations have been observed and demonstrate the utility of low volume HIIT training. It has been suggested to use PPO or vVGO2max as a standard to follow when designing interval programs (5,28). The current study used this approach to more clearly delineate the acute responses to a 60s/60s interval program when different protocols are used. PRACTICAL APPLICATIONS Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 20. Results from the present study quantify the effects of altering either the intensity of the work or the recovery interval when performing interval sessions consisting of 60s of work and 60s of recovery for multiple repetitions. The information provided may aid those interested in designing interval training sessions by providing ranges of values that could be expected for individuals who possess moderate levels of cardiopulmonary fitness. Using a work intensity of 80% or 100% VGO2peak and a recovery intensity of 0% or 50% VGO2peak, subjects were able to exercise within the ACSM recommended range for exercise intensity. Based upon the data it would appear that a protocol such as the 80/0 may be appropriate for those individuals who are just beginning a program or have little experience with interval-type activity. By contrast, a 100/50 protocol could not be completed by all of the subjects and therefore may be too intense for some individuals. Although the 100/0 protocol produced high peak VGO2 values and [bLa], the average VGO2 response was relatively low. On the other hand, a protocol such as 80/50 may allow an individual to sustain a relatively high average %VGO2peak and [bLa] and based upon the average and peak RPE responses most likely be able to complete the training session. From the range of values obtained for VGO2, HR, RPE and [bLa] obtained for the 80/0, 80/50 and 100/0 protocols, it appeared that the use of these protocols would be appropriate for individuals who are at the low to moderate end of the cardiopulmonary fitness spectrum. Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 21. References 1. Allen, DG, Lamb, GD, and Westerblad, H. Skeletal muscle fatigue: cellular mechanisms. Physiol Rev 88: 287-332, 2008. 2. Belcastro, AN, and Bonen, A. Lactic acid removal rates during controlled and uncontrolled recovery exercise. J Appl Physiol 39: 932-936, 1975. 3. BiIlat, LV. Interval training for performance: A scientific and empirical practice. Part 1: aerobic interval training. Sports Med 31: 13-31, 2001. 4. Billat, LV. Interval training for performance: A scientific and empirical practice. Part 2: anaerobic interval training. Sports Med 31: 75-90, 2001. 5. Billat, LV, Slawinski, J, Bocquet, V, Chassaing, P, Demarle, A, and Koralsztein, JP. Very short (15s-15s) interval-training around critical velocity allows middle-aged runners to maintain VGO2max for 14 minutes. Int J Sports Med 22: 201-208, 2001. 6. Billat, LV, Slawinski, J, Bocquet, V, Demarle, A, Lafitte, L, Chassaing, P, and Koralsztein, JP. Intermittent runs at the velocity associated with maximal oxygen uptake enables subjects to remain at maximal oxygen uptake for a longer time than intense but submaximal runs. Eur J Appl Physiology 81: 188-196, 2000. 7. Billat, LV, Petitt, B, and Koralsztein, JP. Time to exhaustion at the velocity associated with VO2max as a new parameter to determine a rational basis for interval training in elite distance runners. Sci Motricite 28: 13-20, 1996. 8. Borg, GAV. Psychosocial bases of perceived exertion. Med Sci Sports Exerc 14: 377-381, 1982. Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 22. 9. Brickley, G, Doust, J, and Williams, CA. Physiological responses during exercise to exhaustion at critical power. Eur J Appl Physiol 88: 146-151, 2002. 10. Brooks, GA, Fahey, TD, White, TP, and Baldwin, KM. Exercise Physiology: Human Bioenergetics and Its Applications (3rd Ed). Mountain View, CA: Mayfield, 2000. p. 462. 11. Burgomaster, KA, Howarth, KR, Philips, SM, Rakobowchuk, M, MacDonald, MJ, McGee, SL, and Gibala, MJ. Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J Physiol 586: 151-160, 2008. 12. Cohen, J. Statistical Power Analysis for the Behavioral Sciences (2nd Ed). New York, NY: LEA Publishers, p. 274. 13. Currie, KD, Dubberly, JB, Mckelvie, RS, and MacDonald, MJ. Low-volume, high intensity interval training in patients with CAD. Med Sci Sports Exerc 45: 1436-1442, 2013. 14. Daniels, J and Scardina, N. Interval training and performance. Sports Med 1: 327-334, 1984. 15. Del Coso, J, Hamouti, N, Aguado-Jimenez, R, and Mora-Rodriguez, R. Restoration of blood pH between repeated bouts of high-intensity exercise: effects of various active- recovery protocols. Eur J Appl Physiol 108: 523-532, 2010. 16. Dupont, G, Moalla, W, Guinhouya, C, Ahmaidi, S, and Berthoin, S. Passive versus active recovery during high-intensity intermittent exercises. Med Sci Sports Exerc. 36:302-308, 2004. 17. Enoka, RM and Duchateau, J. Muscle fatigue: what, why and how it influences muscle function. J Physiol 586: 11-23, 2008. Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 23. 18. Garber, CE, Blissmer, B, Deschenes MR, Franklin, BA, Lamonte, MJ, Lee, IM, Nieman, DC, and Swain DP. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 43: 1334-1359, 2011. 19. Gibala, MJ, Little, JP, Van Essen, M, Wilkin, GP, Burgomaster, KA, Safdar, A, Raha, S, and Tarnopolsky, MA. Short-term sprint interval versus traditional endurance training: similar initial adaptations in human skeletal muscle and exercise performance. J Physiol 575: 901-911, 2006. 20. Gibala, MJ, Little, JP, MacDonald, MJ, and Hawley, JA. Physiological adaptations to low- volume, high intensity interval training in health and disease. J Physiol 590: 1077-1084, 2012. 21. Gist, NH, Fedewa, MV, Dishman, RK, and Cureton, KJ. Sprint interval training effects on aerobic capacity: a systematic review and meta-analysis. Sports Med 44: 269-279, 2014. 22. Guirard, T, Nigam, A, Juneau, M, Meyer, P, Gayda, M, and Bosquet, L. Acute responses to high-intensity intermittent exercise in CHD patients. Med Sci Sports Exerc 43: 211- 217, 2012. 23. Hashimoto, T, Hussien, R, Oommen, S, Gohil, K, and Brooks, GA. Lactate sensitive transcription factor network in L6 cells: activation of MCT1 and mitochondrial biogenesis. FASEB J 21: 2602-2612, 2007. Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 24. 24. Haykowsky, MJ, Timmons, MP, Kruger, C, McNeely, M, Taylor, DA, and Clark, AM. Meta- analysis of aerobic interval training on exercise capacity and systolic function in patients with heart failure and reduced ejection fractions. Am J Cardiol 111: 1466-1469, 2013. 25. Hood, MS, Little, JP, Tarnopolsky, MA, Myslik, F, and Gibala, MJ. Low-volume interval training improves muscle oxidative capacity in sedentary adults. Med Sci Sports Exerc 43: 1849-1856, 2011. 26. Kemi, OJ and Wisloff, U. High intensity aerobic exercise training improves the heart in health and disease. J Cardiopulm Rehab Prev 30: 2-11, 2010. 27. Laursen, PB and Jenkins, DG. The scientific basis for high-intensity interval training. Sports Med 32: 53-73, 2002. 28. Laursen, PB, Shing, CM, Peake, JM, Coombes, JS, and Jenkins, DG. Interval training program optimization in highly trained endurance cyclists. Med Sci Sports Exerc 34: 1801-1807, 2002. 29. Little, JP, Gillen, JB, Percival, ME, Safdar, A, Tarnopolsky, MA, Punthakee, Z, Jung, ME, and Gibala, MJ. Low-volume high-intensity interval training reduces hyperglycemia and increases muscle mitochondrial capacity in patients with type 2 diabetes. J Appl Physiol 111: 1554-1560, 2011. 30. Mathews, DK and Fox, EL. The Physiological Basis of Physical Education and Athletics. Philadelphia, PA: Saunders, 1974. pp. 21-29. 31. McLellan, TM and Skinner, JS. Blood lactate removal during active recovery related to the aerobic threshold. Int J Sport Med 3: 224-229, 1982. Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 25. 32. McMahon, S and Jenkins, D. Factors affecting the rate of phosphocreatine resynthesis following intense exercise. Sports Med 32: 761-784, 2002. 33. Millet, GP, Candau, R, Fattori, P, Bignet, F, and Varray, A. VGO2 responses to different intermittent runs at velocity associated with VGO2max. Can J Appl Physiol. 28:410-423, 2003. 34. Pescatello, LS. ACSM's Guidelines for Exercise Testing and Prescription. Lippincott Williams & Wilkins: Philadelphia, PA, 2014. p. 167. 35. Rozenek, R, Funato, K, Kubo, J, Hoshikawa, M, and Matsuo, A. Physiological responses to interval training sessions at velocities associated with VGO2max. J Strength Cond Res 23: 188-192, 2007. 36. Seiler, S and Sjursen, JE. Effect of work duration on physiological and rating scale of perceived exertion responses during self-paced interval training. Scand J Med Sci Sports 14: 318-325, 2004. 37. Smith, TP, Coombes, JS, and Geraghty, DP. Optimising high-intensity treadmill training using the running speed at maximal O2 uptake and the time for which this can be maintained. Eur J Appl Physiol 89: 337-343, 2003. 38. Spencer, M, Bishop, D, Dawson, B, Goodman, C, and Duffield, R. Metabolism and performance in repeated cycle sprints: active versus passive recovery. Med Sci Sports Exerc 38: 1492-1499, 2006. 39. Stepto, NK, Martin, DT, Fallon, KE, and Hawley, JA. Metabolic demands of intense aerobic interval training in competitive cyclists. Med Sci Sports Exerc 33: 303-310, 2001. Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 26. 40. Tabata, I, Nishimura, K, Kouzaki, M, Hirai, Y, Ogita, F, Miyachi, M, and Yamamoto, K. Effects of moderate intensity-endurance and high-intensity intermittent training on anaerobic capacity and VGO2max. Med Sci Sports Exerc 28: 1327-1330, 1996. 41. Tietz, NW. Textbook of Clinical Chemistry. Philadelphia, PA: Saunders, 1986. pp. 483. 42. Weston, AR, , Myburgh, KH, Lindsay, FH, Dennis, SC, Noakes, TD, and Hawley, JA. Skeletal muscle buffering capacity and endurance performance after high-intensity interval training by well-trained cyclists. Eur J Appl Physiol Occup Physiol 75:7-13, 1997. 43. Weston, M, Taylor, KL, Batterham, AM, and Hopkins, WG. Effects of low-volume high- intensity interval training (HIT) on fitness in adults: a meta-analysis of controlled and non-controlled trials. Sports Med 44: 1005-1017, 2014. 44. Whitehurst, M. High intensity interval training: an alternative for older adults. Am J Lifestyle Med 6: 382-386, 2012. 45. Yoshida, T, Watari, H, and Tagawa, K. Effects of active and passive recoveries on splitting of the inorganic phosphate peak determined by 31P-nuclear magnetic resonance spectroscopy. NMR Biomedicine 9: 13-19; 1996. Acknowledgements The authors wish to thank the dedicated group of participants who volunteered their time and effort to allow this research to be made possible. The results of this present study do not constitute endorsement of any product by the authors or the NSCA. The authors report no conflict of interest with their research. Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 27. Figure Legends Figure 1: Time course for changes in VGO2 expressed as %VGO2peak for each of the four intervals trials. * indicates a difference (p < 0.05) from the first interval. ♦ indicates a difference (p < 0.05) from the fifth interval. (p < 0.05). Between-trial differences in average, peak, and nadir %VGO2peak and 95% confidence intervals can be found in Table 2. Dotted horizontal lines represent ACSM recommended range for exercise intensity. Data points are expressed as a mean + standard deviation. File format: PPT. Figure 2: Time course for changes in HR expressed as %HRpeak for each of the four intervals trials. * indicates a difference (p < 0.05) from the first interval. ♦ indicates a difference (p < 0.05) from the fifth interval. (p < 0.05). Between-trial differences in average, peak, and nadir %HRpeak and 95% confidence intervals can be found in Table 3. Dotted horizontal lines represent ACSM recommended range for exercise intensity. Data points are expressed as a mean + standard deviation. File format: PPT. Figure 3: Time course for changes in blood lactate concentrations [bLa] for each of the four interval trials. * indicates a difference (p < 0.05) from rest. Between-trial [bLa] differences at rest, at the end of the 5th and 10th work interval and 95% confidence intervals can be found in Table 4. Bars are expressed as a mean + standard deviation. File format: PPT. Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 28. Figure 4: Time course for changes in RPE for each of the four intervals trials. * indicates a difference (p < 0.05) from the first interval. Between-trial differences in average, peak, and nadir RPE and 95% confidence intervals can be found in Table 5. Dotted horizontal lines represent ACSM recommended range for exercise intensity. Data points are expressed as a mean + standard deviation. Data points are expressed as a mean + standard deviation. File format: PPT. Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 29. Tables Table 1: Physical Characteristics of Subjects. Values are expressed as a mean + the standard deviation. Subjects (n) Age (yr) Height (cm) Mass (kg) Body Fat (%) VGO2peak (ml x min-1 x kg-1 ) HRpeak (b x min-1 ) PPO (W) Pre-GXT [bLa] (mmol x l-1 ) Post-GXT [bLa] (mmol x l-1 ) 5 Males 28.0 ± 5.8 178.0 ± 7.3* 75.6 ± 7.6* 13.6 ± 4.8* 51.8 ± 10.0 181.6 ± 6.9 278.0 ± 13.0* 1.4 ± 0.9 13.4 ± 3.8 6 Females 24.3 ± 4.6 164.7 ± 6.2 59.0 ± 6.7 24.5 ± 5.0 45.8 ± 8.7 182.5 ± 6.2 200.0 ± 34.6 1.2 ± 0.4 10.3 ± 2.2 11 Total 26.0 ± 5.3 170.7 ± 9.4 66.5 ± 11.0 19.5 ± 7.3 48.5 ± 9.4 182.1 ± 6.2 235.5 ± 48.2 1.3 ± 0.6 11.7 ± 3.1 * = males different than females (p < 0.05). Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 30. Acute Responses to Various HIIT protocols 2 Table 2: Oxygen uptake expressed as a percentage of VGO2peak (%VGO2peak) obtained from the GXT. Values represent averages across all intervals within a trial expressed as a mean + the standard deviation. 95% Confidence Intervals Trial %VGO2peak Lower Upper 80/0 54.8 ± 6.5b c d 50.4 59.2 80/50 74.7 ± 8.7a c d 68.8 80.5 100/0 65.4 ± 9.0a b d 59.4 71.4 Average 100/50 82.8 ± 6.2a b c 78.6 86.9 80/0 67.5 ± 6.3b c d 63.2 71.7 80/50 79.8 ± 8.8a d 73.9 85.7 100/0 80.9 ± 8.7a d 75.0 86.7 Peak 100/50 90.2 ± 6.6a b c 85.7 94.6 80/0 43.6 ± 7.5 b c d 38.5 48.6 80/50 72.6 ± 8.9a c d 66.5 78.5 100/0 51.7 ± 9.9a b d 45.0 58.3 Nadir 100/50 78.9 ± 7.3a b c 73.9 83.8 a = Trial was different from 80/0 (p < 0.05). b = Trial was different from 80/50 (p < 0.05). c = Trial was different from 100/0 (p < 0.05). d = Trial was different from 100/50 (p < 0.05). Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 31. Acute Responses to Various HIIT protocols 3 Table 3: Heart rate expressed as a percentage of HRpeak (%HRpeak) obtained from the GXT. Values represent averages across all intervals within a trial expressed as a mean + the standard deviation. 95% Confidence Intervals Trial %HRpeak Lower Upper 80/0 74.9 ± 7.1 b c d 70.2 79.7 80/50 86.1 ± 6.6a c 81.7 90.6 100/0 83.2 ± 7.2 b d 78.3 88.1 Average 100/50 90.9 ± 3.8a c 88.3 93.4 80/0 83.2 ± 5.5 b c d 79.5 87.0 80/50 88.8 ± 5.9a d 84.9 92.8 100/0 90.0 ± 5.5 a d 86.3 93.7 Peak 100/50 94.6 ± 3.0 a b c 92.5 96.6 80/0 67.8 ± 10.2 b c d 60.9 74.7 80/50 85.3 ± 7.3 a c 80.4 90.3 100/0 77.5 ± 9.9 a b d 70.8 84.2 Nadir 100/50 89.8 ± 5.2 a c 86.3 93.3 a = Trial was different from 80/0 (p < 0.05). b = Trial was different from 80/50 (p < 0.05). c = Trial was different from 100/0 (p < 0.05). d = Trial was different from 100/50 (p < 0.05). Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 32. Acute Responses to Various HIIT protocols 4 Table 4: Blood lactate concentration [bLa] obtained at rest at the end of the fifth and tenth work intervals. Values expressed as a mean ± the standard deviation. 95% Confidence Intervals Trial [bLa] Lower Upper GXT 1.3 + 0.8 0.7 1.8 80/0 1.4 + 0.7 0.9 1.9 80/50 1.5 + 0.5 1.2 1.8 100/0 1.2 + 0.5 0.8 1.5 Rest 100/50 1.2 + 0.3 1.0 1.4 80/0 4.9 + 1.9 c d 3.6 6.2 80/50 6.8 + 2.6 d 5.0 8.6 100/0 8.5 + 2.3 a 6.9 10.0 End of 5th Work Interval 100/50 10.5 + 3.0 a b 8.5 12.5 GXT 11.8 + 3.1 a b 9.7 13.9 80/0 5.0 + 2.4 c d e 3.4 6.6 80/50 7.4 + 2.8e 5.5 9.3 100/0 9.6 + 3.6 a 7.2 12.0 End of 10th Work Interval 100/50 10.2 + 2.7 a 7.9 12.5 a = Trial was different from 80/0 (p < 0.05). b = Trial was different from 80/50 (p < 0.05). c = Trial was different from 100/0 (p < 0.05). d = Trial was different from 100/50 (p < 0.05). e = Trial was different from GXT (p < 0.05). Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 33. Acute Responses to Various HIIT protocols 5 Table 5: RPE obtained from all trials. Values represent averages across all intervals within a trial expressed as a mean + the standard deviation. 95% Confidence Intervals Trial RPE Lower Upper 80/0 10.5 ± 1.3 b c d 9.6 11.4 80/50 13.4 ± 1.7 a 12.3 14.6 100/0 12.5 ± 1.7 a d 11.3 13.6 Average 100/50 14.3 ± 1.8 a c 13.1 15.5 80/0 12.6 ± 1.1 b c d 11.8 13.4 80/50 14.3 ± 1.5 a d 13.4 15.3 100/0 14.9 ± 1.4 a d 13.9 15.8 Peak 100/50 15.7 ± 1.2 a b c 14.8 16.4 80/0 8.4 ± 1.9 b d 7.0 9.7 80/50 12.4 ± 2.2 a c 11.0 13.9 100/0 10.0 ± 2.3 b d 8.5 11.6 Nadir 100/50 12.8 ± 2.5a c 11.1 14.5 a = Trial was different from 80/0 (p < 0.05). b = Trial was different from 80/50 (p < 0.05). c = Trial was different from 100/0 (p < 0.05). d = Trial was different from 100/50 (p < 0.05). Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 34. Trial 1 2 3 4 5 6 7 8 9 10 * ¨ * * ** * * * ¨* * * * Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 35. Trial 1 2 3 4 5 6 7 8 9 10 ¨ * * * * ** * * * * * ¨ ¨ ¨ ¨ ¨ ¨ ¨ * Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 36. * ** * * * * * * Copyright ª 2016 National Strength and Conditioning Association A C C EPTED
- 37. Trial 1 2 3 4 5 6 7 8 9 10 * * * * * * * * * * * * Copyright ª 2016 National Strength and Conditioning Association A C C EPTED