3. Twelve Members of vitamin B complex
1. B1- Thiamine
2. B2- Riboflavin
3. B3- Niacin
4. B6- Pyridoxine
5. B12- Cyanocobalamin
6. B9 - Folic Acid
7. Para amino benzoic acid
8. B5 -Pantothenic acid
9. Lipoic acid
10. B7- Biotin
11. Choline
12. Inositol ( F, P, P,L B C I)
grouped together because all of them function
as coenzymes in the human cells.
4. Properties of B complex vitamins
❖Properties of B complex vitamins are :
1. Water soluble
2. Yellow colored
3. Coenzymes
4. Synthesized by gastrointestinal bacteria
5. Non toxic
5. Sources of B complex vitamins
• Sources of B complex vitamins include
a. Germinating seeds
b. aleurone layer of cereals ( food grains –e.g. rice ,wheat )
c. wheat germ
d. Pulses
e. beans
f. Fruits
g. Yeast
h. Liver
i. Meat
j. Egg
6. ❖ Aleurone layer of cereals is rich source of thiamine.
❖ When grains are polished , aleurone layer of cereals is removed .
❖ Whole wheat flour and unpolished rice have better nutritive value than completely
polished refined food .
Aleurone layer of cereals as dietary source of B complex vitamins
7. Recommended daily allowance of B complex vitamins
B complex vitamin Recommended daily allowance of B complex( adults)
B1 -Thiamine 1.0-1.5 mg
B2- Riboflavin 1.5 mg
B3- Niacin 20 mg
B6- Pyridoxine 2 mg
B12- Cyanocobalamin 1.0 microgram
B9 - Folic Acid 100 microgram
Para amino benzoic acid 10 mg
B5 -Pantothenic acid 10 mg
B7- Biotin 200 micrograms
Choline Synthesized in human body by intestinal bacteria
(400mg)
9. Vitamin Coenzyme form Functions
Thiamine –B1 Thiamine pyrophosphate- TPP Carbohydratemetabolism,Oxidative
Decarboxylationofalphaketoacids
Riboflavin-B2 Flavin monophosphate- FMN
Flavin adenine dinucleotide -FAD
Oxidation ,reduction reactions
Oxidized in ETC (1.5 ATP)
Nicotinic acid B3 Nicotinic adenine dinucleotide -
NAD+ Nicotinic adenine dinucleotide
Phosphate -NADP+
Oxidation ,reduction reactions
Oxidized in ETC (2.5ATP),
hydroxylation reactions
PantothenicacidsB5 Coenzyme A - CoA Fattyacidssynthesis–fattyacidCoA
Pyridoxine –B6 Pyridoxal ,pyridoxamine, Pyridoxine Amino group transfer
Biotin- B7 Biocytin CO2 transfer
Folic acid -B9 Tetra hydro folic acid FH4 1-C transfer
Cyanocobalamin-
B12
methyl cobalamin ,Deoxy adenosyl
cobalamin
IsomerizationofmethylmalonylCoA,
methylationofhomocysteine
Coenzyme forms and Functions of Vitamin B complex
10. Biochemical manifestations of Vitamin B complex deficiency
❖Biochemical manifestations of Vitamin B complex deficiency include
decreased
• rate of TCA
• amino acid synthesis
• protein biosynthesis impaired anabolism in the human body.
• lipid synthesis
• gluconeogenesis
❖ This leads to Inadequate growth, Loss of weight , strength and apathy (due
to decreased ATP synthesis).
11. Deficiency manifestation of vitamin B complex: 1
1. Inadequate growth
2. Loss of weight & strength (due to decreased ATP synthesis)
3. Microcytic ,Hypochromic anemia (as availability of succinyl CoA
decreases →decreased heme )
4. Neurological manifestations include
a) Loss of memory
b) Apathy
c) Numbness ( pins and needles sensation in legs)
Neurological manifestations due to decreased availability of acetyl CoA and
NADPH resulting in decreased fatty acid synthesis.
5. Decreased Trp pyrrolase activity resulting in decreased synthesis of
neurotransmitter Acetyl choline ( in Kynurenine pathway Trp is oxidized
Kynurenine which converted to Acetyl CoA or niacin. Acetyl CoA is a
precursor for Acetyl choline synthesis ).
15. Structure and chemistry of Thiamine
❖Adolf Windaus (Noble 1928)- elucidated structure of thiamine.
Thiamine contains a substituted pyrimidine ring connected to a
substituted Thiazole ring by means of methylene bridge.
▪ Christian Eijkman (Noble 1929)- produced Beriberi in chicken by
feeding polished rice.
• Thiamine ( Vitamin B1) Thymine (is base present in DNA)
• Active form of Thiamine is Thiamine Pyrophosphate (TPP).
Thiamine + ATP → Thiamine Pyrophosphate (TPP)+ AMP (catalyzed by
TPP transferase in the jejunal mucosa)
17. Activation of Thiamine to Thiamine phosphate
ActivationofThiaminetoThiaminephosphate(TPP)iscatalyzedbyThiaminepyrophosphatetransferase
whichtransfers twophosphategroupsofATPinthejejunalmucosa.
substitutedThiazolering
methylene bridge
substituted pyrimidine ring
18. Properties of Thiamine (vitamin B1 )
❖Properties of Thiamine (vitamin B1 ) :
1. Water soluble
2. Yellow colored
3. Coenzymes
4. Synthesized by gastrointestinal bacteria
5. Non toxic
6. Stable in acid medium
7. Destroyed in an alkaline medium even at room temperature and by
improper cooking .
8. Cleaved into pyrimidine and thioazole half at p H 5 in sodium bisulphite
solution
9. oxidized with potassium ferricyanide in alkaline solution to thiochrome
which has strong fluorescence ( estimation of Thiamine using fluorometry)
10. Destroyed when autoclaved at 120 C for 30 minutes.
20. Recommended dietary allowance (RDA)of Thiamine (vitamin B1)
Category Recommended dietary allowance of Thiamine
(vitamin B1)
Adults 1.0 - 1.5 mg /day ( 0.5 mg/1000 Cal)
Children 0.7 -1.2 mg /day
Pregnant and lactating 2 mg /day
Old age and alcoholics 2 mg /day
Therapeutic doses : 5 – 20 mg of Thiamine daily have been proved to be beneficial .
Thiamine requirement is related to energy metabolism and therefore are expressed
in terms of energy.
21. Metabolism of Thiamine /Vitamin B 1/Antiberiberi factor/Antineuritis
Metabolism of Thiamine :
1. Absorption of Thiamine in small intestine:
➢ Dietary Thiamine is readily absorbed in the small intestine by a carrier
mediated active transport process as long as intake is less than 5mg/day .
At higher intake levels passive diffusion contributes to absorption.
➢ It is then phosphorylated to its active form TPP in the jejunal mucosa
by enzyme thiamine pyrophosphate transferase .
➢ Thiamine is carried by portal blood to the liver after its absorption..
2. The free vitamin occurs in the blood and coenzyme form TPP
predominates in the cellular component.
3. No storage of Thiamine in human body therefore its regular supplies
needed in diet to maintain blood levels .
4. 10% excretion in urine along with its several catabolites .
22. Coenzyme role of Thiamine Pyrophosphate
❖Thiamine is required mainly for carbohydrate metabolism.
❖Thiamine in the form of its coenzyme Thiamine Pyrophosphate is
involved in the following enzymatic reactions :
1 . Oxidative decarboxylation in
a) Pyruvate dehydrogenase complex
b) Alpha ketoglutarate dehydrogenase complex
c) Alpha Keto Acid Dehydrogenase complex of branched chain alpha keto
acids of Valine ,Leucine, Isoleucine )
2. Transketolation by Transketolases in hexosemonophosphatepathway/shunt
ofGlucose
23. Pyruvate Dehydrogenase Complex
❖ Pyruvate Dehydrogenase Complex has three enzymes :
1. Pyruvate Dehydrogenase
2. Dihydrolipoyl Dehydrogenase
3. Dihydrolipoyl Transacetylase
❖ Pyruvate Dehydrogenase Complex has five coenzymes :
1) TPP
2) FAD
3) NAD+
4) CoA SH
5) Lipoic acid
❖Pyruvate Dehydrogenase Complex uses Magnesium (Mg 2+) as a
cofactor.
24. Biochemical Functions of Thiamine :1
Pyruvate Dehydrogenase catalyzes oxidative decarboxylation of Pyruvate to Acetyl CoA (used
in TCA) and carbon dioxide. TPP functions as a coenzyme in this reaction.( cocarboxylase )
Coenzyme role of TPP in Pyruvate Dehydrogenase Complex
25. Role of Thiamine in Neural functions via Acetyl CoA
❖TPP is a coenzyme for Pyruvate Dehydrogenase Complex which catalyzes oxidative decarboxylation
of Pyruvate to Acetyl CoA and carbon dioxide.
❖ Acetyl CoA is involved in synthesis of :
1. Intermediates of TCA cycle → ATP ( essential for brain )
2. Neurotransmitter acetyl choline
3. Cholesterol ( as an insulating cover of nerve fibers for transmission of electrical impulses in the nervous
tissue )
4. Fatty acid ( Docosa-hexanoic acid DHA 3- cervonic acid is needed for development of brain,
sulphogalactoceramide found in myelin )
5. N- acetylneuraminic acid →ganglioside ( found on the nerve endings for binding of neurotransmitters
during neve impulse transmission )
6. Myelin (sphingomyelins are important constituent of brain and nervous tissue )
7. Acetylated amino sugars (N-acetylglucosamine, N-acetyl galactosamine are needed to prevent mental
retardation – mucopolysaccharidoses )
8. N-acetyl glutamate (NAG) in urea biosynthesis (needed to prevent toxic effects of ammonia on brain )
9. Glucose (brain tissue normally uses glucose as an exclusive fuel except during starvation . Human
brain needs 120 gm /day out of 160 gm needed by entire body for continuous supply of energy .Acetyl
CoA is activator of pyruvate carboxylase and promotes gluconeogenesis during starvation. )
10. Acetic acid (Acetyl CoA is active form of Acetic acid which is involved in conjugation of isoniazid during
Xenobiotic metabolism. Failure of this reaction leads to psychosis in tuberculosis patients
➢ Conclusion : Thiamine and Acetyl CoA are required for the normal functioning of the nervous system.
26. Thiaminedeficiencyandbiochemicalchangesin PyruvateDehydrogenaseComplex
❖Biochemicalchangesin PyruvateDehydrogenaseComplexIn Thiaminedeficiency
areasfollows :
➢Decreased Pyruvate Dehydrogenase Activity( impairment in
conversion of Pyruvate to Acetyl CoA ) → Increased plasma Pyruvate
concentration and its excretion in urine. Accumulation of Pyruvate
occurs in tissues which is harmful.
➢ Normally Pyruvate does not cross the blood brain barrier and enter
the brain. However, in Thiamine deficiency ,alteration occurs in the
blood brain barrier permitting Pyruvate to enter the brain directly .
➢Pyruvate accumulation in brain results in its disturbed metabolism
and may be responsible for polyneuritis.
➢Lactic acidosis (Increased plasma Pyruvate concentration→ Increased
plasma lactate concentration )
27. Coenzyme role of TPP in Alpha ketoglutarate dehydrogenase complex
Alpha ketoglutarate dehydrogenase catalyzes oxidative decarboxylation of Alpha ketoglutarate to
succinyl CoA and carbon dioxide (in TCA).TPP functions as a coenzyme in this reaction( cocarboxylase ).
Biochemical Functions of Thiamine :2
28. Thiamine deficiency and Alpha ketoglutarate dehydrogenase
complex
• TPP is a coenzyme for Alpha ketoglutarate dehydrogenase which
catalyzes oxidative decarboxylation of Alpha ketoglutarate to succinyl CoA
and carbon dioxide (in TCA).
• Thiamine deficiency leads to malfunctioning of TCA ( defective energy
metabolism) and Microcytic ,Hypochromic anemia (as the availability of
succinyl CoA decreases →decreased heme synthesis ).
31. Coenzyme role of TPP with Transketolases in hexose monophosphate
shunt of Glucose:2
Hexose monophosphate shunt of Glucose is involved in synthesis of ribose 5 phosphate (synthesis of
nucleic acids )and NADPH (synthesis of fatty acids ,steroids ,neurotransmitters ,reduced glutathione)
32. Thiamine deficiency and Transketolases in hexose monophosphate shunt of
Glucose
• In Thiamine deficiency ,the activity of TPP dependent transketolases in
hexose monophosphate shunt of Glucose is impaired .
• Impaired activity of TPP dependent transketolases results in impaired
synthesis of ribose 5 phosphate (hence impaired synthesis of nucleic
acids )and NADPH (impaired synthesis of fatty acids ,steroids,
neurotransmitters ,reduced glutathione) .
➢Impaired activity of TPP dependent transketolases leads to neurological
manifestations.
33. Coenzyme role of TPP in Alpha Keto Acid Dehydrogenase complex of
branched chain alpha keto acids :1
(uses coenzymes –TPP , NAD+, FAD+, Lipoic acid and Mg 2 +as a cofactor )
34. ❖branched chain alpha keto acids of Valine ,Leucine, Isoleucine are .
ketoisovalerate, ketoisocaproate , keto - -methyl valerate
( corresponding ketoacids of Valine ,Leucine, Isoleucine )
+
Alpha Keto Acid Dehydrogenase complex
(uses coenzymes –TPP , NAD+, FAD, Lipoic acid and Mg 2 +as a cofactor )
Transfer of activated CHO group to Alpha Lipoic Acid
Isobutyryl CoA , isovaleryl CoA , methylbutyryl CoA
( corresponding , unsaturated acyl CoA thioesters)
Coenzyme role of TPP in Alpha Keto Acid Dehydrogenase complex of
branched chain alpha keto acids :2
Alpha Keto Acid Dehydrogenase catalyzes oxidative decarboxylation of ketoacids to , unsaturated
acyl CoA thioesters and carbon dioxide .TPP functions as a coenzyme in this reaction.
35. Thiamine deficiency and Alpha Keto Acid Dehydrogenase complex
• Branched chain amino acids viz Valine ,Leucine, Isoleucine
undergo transamination reaction to corresponding branched chain
alpha keto acids ketoisovalerate, ketoisocaproate , keto - -
methyl valerate. These are then converted to Acetyl CoA through
Alpha Keto Acid Dehydrogenase complex which uses TPP as a
coenzyme. .
• In Thiamine deficiency , the activity of Alpha Keto Acid
Dehydrogenase complex is impaired .This results in accumulation
of Valine ,Leucine, Isoleucine and their corresponding branched
chain alpha keto acids in blood ,urine CSF ( condition similar to
maple syrup urine) .
• In Thiamine deficiency ,synthesis of Acetyl CoA is impaired
through this pathway , this leads to neurological manifestations .
36. Thiamine deficiency and impaired cellular functions
• Thiamine deficiency leads to failure of carbohydrate metabolism
,resulting in deceased production of ATP and impaired cellular
functions of central nervous system ( peripheral nerves and
brain),heart and gastrointestinal tract.
• The overall picture of thiamine deficiency including cardiovascular,
neurological and gastrointestinal disorders is referred as Beriberi.
37. Cardio vascular manifestations in Thiamine deficiency
• Cardio vascular manifestations in Thiamine deficiency are
1. Palpitation/increase in heart rate (tachycardia)
2. enlargement of heart ( cardiomegaly, Hypertrophy)
3. Dilatation
4. Cardiac failure
5. Edema
39. Cardiac failure in Thiamine deficiency
Thiamine deficiency
failure of carbohydrate metabolism ,resulting in deceased production of ATP
Demand for oxygen supply by peripheral tissue for synthesis of ATP(through
biological oxidation involving ETC and oxidative phosphorylation )
Palpitation/increase in heart rate (→tachycardia) to fulfil increased oxygen
demand by the peripheral tissue
Enlargement of heart ( cardiomegaly, Hypertrophy , heart is a muscle )
Vein efforts of heart for oxygen supply to peripheral tissue due to microcytic, Hypochromic
anemia (as availability of succinyl CoA decreases →decreased heme )
Cardiac failure → renal failure→ Edema
40. Cardiac failure in Thiamine deficiency
Thiamine deficiency →Cyanosis →due to increased oxygen consumption
/demand by peripheral tissue
41. Neurological manifestations in Thiamine deficiency
❖Neurological manifestations include :
a. anxiety
b. mental confusion
c. motor and sensory neuropathy ( Wernicke ’s encephalopathy )
d. peripheral neuritis
❖Neurological manifestations are due to
1. decreased availability of acetyl CoA and NADPH resulting in decreased fatty
acid synthesis.
2. Decreased Tryptophan pyrrolase activity resulting in decreased synthesis of
neurotransmitter Acetyl choline ( in Kynurenine pathway Trp is oxidized
Kynurenine by Tryptophan pyrrolase using TPP as a coenzyme . Kynurenine is
then converted to Acetyl CoA or niacin. Acetyl CoA is a precursor in Acetyl
choline synthesis . )
3. decreased transketolase activity (resulting in impaired synthesis of NADPH
hence impaired synthesis of fatty acids ,steroids ,neurotransmitters , reduced
glutathione).
42. Role of Thiamine in Neural functions via Acetyl CoA
❖TPP is a coenzyme for Pyruvate Dehydrogenase Complex which catalyzes oxidative decarboxylation
of Pyruvate to Acetyl CoA and carbon dioxide.
❖ Acetyl CoA is involved in synthesis of :
1. Intermediates of TCA cycle → ATP ( essential for brain )
2. Neurotransmitter acetyl choline
3. Cholesterol ( as an insulating cover of nerve fibers for transmission of electrical impulses in the nervous
tissue )
4. Fatty acid ( Docosa-hexanoic acid DHA 3- cervonic acid is needed for development of brain,
sulphogalactoceramide found in myelin )
5. N- acetylneuraminic acid →ganglioside ( found on the nerve endings for binding of neurotransmitters
during neve impulse transmission )
6. Myelin (sphingomyelins are important constituent of brain and nervous tissue )
7. Acetylated amino sugars (N-acetylglucosamine, N-acetyl galactosamine are needed to prevent mental
retardation – mucopolysaccharidoses )
8. N-acetyl glutamate (NAG) in urea biosynthesis (needed to prevent toxic effects of ammonia on brain )
9. Glucose (brain tissue normally uses glucose as an exclusive fuel except during starvation . Human
brain needs 120 gm /day out of 160 gm needed by entire body for continuous supply of energy .Acetyl
CoA is activator of pyruvate carboxylase and promotes gluconeogenesis during starvation. )
10. Acetic acid (Acetyl CoA is active form of Acetic acid which is involved in conjugation of isoniazid during
Xenobiotic metabolism. Failure of this reaction leads to psychosis in tuberculosis patients
➢ Conclusion : Thiamine and Acetyl CoA are required for the normal functioning of the nervous system.
43. Gastrointestinal manifestations in Thiamine deficiency
In thiamine deficiency , impaired cellular functions of the
gastrointestinal tract leads to impaired digestion ,constipation and
anorexia (loss of appetite ) .
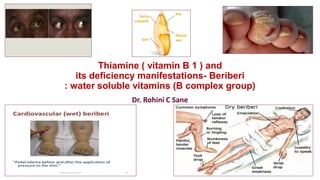
44. Beriberi : Deficiency manifestation of Thiamine
❖Deficiency manifestation of Thiamine→ Beriberi (Singhalese word meaning
weakness/ I cannot ) .
❖ Beriberi has
a. Cardiovascular manifestations
b. Neurological manifestations
c. Gastrointestinal symptoms
❖Types of Beriberi
a) Wet beriberi ( seen when Thiamine deficiency is severe)
b) Dry beriberi ( occurs in chronic dietary deficiency of Thiamine)
c) Infantile beriberi (occurs in infants born to mothers suffering Thiamine
Deficiency)
d) Wernicke- Korsakoff syndrome - cerebral Beriberi (seen in alcoholics with
chronic deficiency of Thiamine )
❖Polyneuritis
45. Wet beriberi : Deficiency manifestation of Thiamine
❖ Wet beriberi seen when Thiamine deficiency is severe.
❖Cardio vascular manifestations of wet beriberi
1. increase in Pulse , palpitation and Heart rate ( tachycardia)
2. Heart becomes weak
3. Breathlessness
4. Edema of legs ,face ,trunk and serous cavity
5. Dilatation, Death occurs due to cardiac /heart failure
❖ Neurological manifestation (due to decreased transketolase activity) :
a. anxiety
b. mental confusion
c. motor and sensory neuropathy ( Wernicke ’s encephalopathy )
d. peripheral neuritis
47. Dry beriberi : Deficiency manifestation of Thiamine
Dry beriberi occurs in chronic dietary deficiency of Thiamine (diet chronically
contains slightly less than Thiamine requirement ) .
❑Manifestation of Dry beriberi :
❖anorexia (loss of appetite )
❖loss of weight
❖Muscular weakness ,Muscle wasting ( walking becomes difficult due to increased
concentration of pyruvic acid & lactic acid)
❖Neurological manifestation (due to decreased transketolase activity is a major
feature) :
a. anxiety
b. mental confusion
c. motor and sensory neuropathy ( Wernicke ’s encephalopathy )
d. peripheral neuritis
49. Infantile beriberi
❖Infantile beriberi occurs in infants born to mothers suffering thiamine
deficiency. The breast milk of mothers of these infants contains low thiamine
content .
❖Symptoms of Infantile beriberi:
1. Restlessness
2. Sleeplessness
3. Anorexia
4. Vomiting
5. Convulsions
6. Edema
7. Tachycardia , Bouts of screaming due to cardiac dilatation
8. Aphonia (absences or loss of voice)
9. If not treated ,death
54. Wernicke-Korsakoff syndrome: Deficiency manifestations of Thiamine
❖ Wernicke- Korsakoff syndrome (seen in alcoholics with chronic deficiency of
Thiamine ). It is also called a cerebral Beriberi .
❖Carl Wernicke (in 1984) and Sergei Sergeivich Korsakoff (in 1987) described this
condition .
❖ Gastrointestinal symptoms in Wernicke- Korsakoff syndrome are due to
1. Decreased intake of diet (including Thiamine) in alcoholics
2. Impaired Gastrointestinal absorption of diet (including Thiamine) (epithelium is
disintegrated in alcoholism)
3. Alcohol inhibits intestinal absorption of Thiamine.
❖ Neurological manifestation (due to decreased transketolase activity)
include Encephalopathy ( Ophthalmoplegia- paralysis of extraocular ,iris , ciliary
muscles→ loss of paired movement of eyes → double vision , Nystagmus- Rapid
back and forth involuntary movements of eyes, Ataxia- defective muscular
coordination →shaky movements )
anorexia ,muscular weakness, peripheral paralysis, Apathy .
If not treated ,it progresses to Korsakoff ’s psychosis which is irreversible and
characterized by loss of memory of recent events, mental confusion, inability to
retain new information.
56. Biochemical changes in Thiamine (Vitamin B1) deficiency:1
❖Biochemical changes in Vitamin B 1 deficiency include decreased
• rate of TCA
• amino acid synthesis
• protein biosynthesis impaired anabolism in the human body.
• lipid synthesis
• gluconeogenesis
❖ This leads to Inadequate growth, Loss of weight & strength (due to
decreased ATP synthesis).
57. Biochemical changes in Thiamine deficiency :2
➢Decreased Pyruvate Dehydrogenase Activity( impairment in conversion of Pyruvate to
Acetyl CoA ) → Increased plasma Pyruvate concentration and its excretion in urine.
Accumulation of Pyruvate occurs in tissues which is harmful.
➢ Normally Pyruvate does not cross the blood brain barrier and enter the brain.
However, in Thiamine deficiency ,alteration occurs in the blood brain barrier permitting
Pyruvate to enter the brain directly .
➢Pyruvate accumulation in brain results in its disturbed metabolism and may be
responsible for polyneuritis.
➢Lactic acidosis (Increased plasma Pyruvate concentration→ Increased plasma lactate
concentration )
❖Decreased Alpha Ketoglutarate dehydrogenase Activity→ Increased plasma Alpha
Ketoglutarate concentration
❑ Transketolase activity decreased → POLYNEURITIS
❑RBC Transketolase activity decreased ( earliest manifestation)
✓Branched chain ketoaciduria with poor activity of the keto acid dehydrogenase system
58. Erythrocyte Transketolase activity : a diagnostic test to assess
Thiamine deficiency.
• Measurement of whole blood /erythrocyte (RBC) Transketolase
activity is a diagnostic test to assess Thiamine deficiency.
❖Reference interval for transketolase activity :
Whole blood Transketolase activity = 9 -12 micromoles /hour/ml
( 150- 200 U/ L)
Erythrocyte Transketolase activity 0.75 – 1.30 U/ g of hemoglobin
60. Thiamine deficiency due to Thiaminase and Pyrithiamine
❖Thiamine deficiency due to Thiaminase from sea food:
Thiamine
Thiaminase (sea food) hydrolysis of thiamine
Pyrimidine + Thiazole
➢ Beriberi is attributed to the consumption of a raw fish (rich in
Thiaminase) in some parts of Japan.
❖Thiamine deficiency due to Pyrithiamine from ferns :
Pyrithiamine is structural analogues / antagonist of Thiamine and inhibits
its activity .
➢Horses and cattle often develop Thiamine deficiency due overconsumption
of the plant fern ( fern poisoning).
❖Oxythiamine is also a structural analogues of Thiamine.
61. Polyneuritis : Deficiency manifestation of Thiamine
❖Polyneuritis be associated with
a) Chronic alcoholics: Alcohol inhibits intestinal absorption of Thiamine .
Polyneuritis is common in chronic alcoholics .
b) Pregnancy: insufficient intake and increased requirement of diet
including Thiamine
c) Old age : insufficient intake of diet including Thiamine, Impaired
Gastrointestinal absorption of diet including Thiamine (epithelium is
disintegrated-degenerative changes )
d) Diabetes Mellitus
❖Thiamine supplementation is beneficial in Polyneuritis.
❖A Lipid soluble acylated derivative ( benfotiamine ) is recommended
to improve diabetic neuropathy. It decreases glycation of proteins
(AGE).