

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Calcium
Similaire à Calcium (20)
Plus de DR RML DELHI
Plus de DR RML DELHI (20)
Dernier
Dernier (20)
Calcium
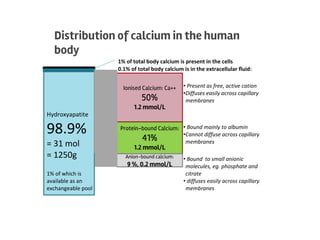
- 1. Distribution of calcium in the human body Hydroxyapatite 98.9% = 31 mol = 1250g 1% of which is available as an exchangeable pool 0.1% of total body calcium is in the extracellular fluid: Ionised Calcium: Ca++ 50% 1.2 mmol/L 1% of total body calcium is present in the cells Protein-bound Calcium: 41% 1.2 mmol/L Anion-bound calcium: 9 %, 0.2 mmol/L • Present as free, active cation •Diffuses easily across capillary membranes • Bound mainly to albumin •Cannot diffuse across capillary membranes • Bound to small anionic molecules, eg. phosphate and citrate • diffuses easily across capillary membranes
- 3. CALCIUM HOMEOSTASIS Hormone Effect Bone Gut Kidney PTH ↑ Ca ↓ Po4 Increases Osteoclasts Indirect via Vit. D Ca reab Po4 exr. Vitamin D3 ↑ Ca ↑ Po4 No direct action ↑ Ca ↑ Po4 absorption No direct effect Calcitonin ↓ Ca ↓ Po4 Inhibits Osteoclasts No direct effect Ca & Po4 excretion 3
- 4. ▶Mild: Total Ca 10.5-11.9 mg/dL or Ionized Ca 1.4-2 mmol/L ▶Moderate: Ca 12-13.9 mg/dL or Ionized Ca 2-2.5 mmol/L ▶Hypercalcemic crisis: Ca 14-16 mg/dL or Ionized Ca 2.5-3 mmol/L HYPERCALCEMIA
- 5. Hypercalcemia - Clinical STONES BONES GROANSMOANS 5 RENAL stones Polyuria , Nocturia failure Bone pain Fracture risk GIT Constipatio n, Nausea Anorexia, Pancreatitis Gastric ulcer CNS Lethargy, Weakness Deppression Confusion, Coma
- 6. CAUSES and Diagnostic Approach ✓PTH ↑ PRIMARY HYPERPARATHYROIDISM TERTIARY HYPERPARATHYROIDISM FHH ✓urine Ca ↑ (>200mg/day) 1° ↑PTH ↓ (<100mg/day) FHH ↓ Non-PTHmediated ✓ PTHrp & Vitamin D ↑ PTHrp Look for cancer BREAST LUNG MYELOMQA ↑ 1,25D (Lymphoma , Granulomat ous disease) EXCESS INTAKE NormalVIT Dand PTHrp THYROTOXICOSIS ADRENAL INSUF RENAL FAILURE IMMOBILISATION DRUGS
- 7. ECG
- 8. ▶Mild, asymptomatic hypercalcemia do not require immediate therapy, and manage underlying cause. ▶ Symptomatic hypercalcemia requires therapeutic intervention ▶ Initial therapy - volume expansion because hypercalcemia invariably leads to dehydration ▶ 4–6 L of i/v saline may be required over the first 24 h ▶ Loop diuretics - enhance sodium and calcium excretion. . Treatment
- 9. In hypercalcemia of malignancy drugs that inhibit bone resorption should be considered. ▶Zoledronic acid (e.g., 4 mg I/V over 30 min) ▶Pamidronate ,Etidronate ▶Onset of action is within 1–3 days. Because of their effectiveness, bisphosphonates have replaced calcitonin widely ▶In rare instances, dialysis may be necessary.
- 10. ▶I/V phosphate may be used, it can be toxic , ca-po4 complexes cause extensive organ damage. ▶In 1,25(OH) D-mediated hypercalcemia- oral or i/v steroids preffered ,decrease 1,25(OH) D production. ▶Recently, US FDA approved denosumab (RANKL inhibitor) for treatment of hypercalcemia of malignancy refractory to bisphosphonate therapy in December 2014
- 11. ▶Serum ca < 8.5 mg/dL or an ionized ca <1.0 mmol/L ▶ Ionized ca is the definitive method for diagnosis ▶ Corrected ca(mg%) = serum ca + (4.0 - albumin g%) x 0.8 Hypocalcemia
- 12. Cardiovascular effects : ▶acute hypocalcemia - syncope, CHF, and angina Neuromuscular symptoms : ▶Numbness and tingling sensations - perioral area or in the fingers and toes ▶Muscle cramps, in the back and lower extremities; may progress to carpopedal spasm (ie, tetany) ▶Wheezing ,Dysphagia,Voice changes History
- 13. Neurologic symptoms : ▶Irritability, impaired intellectual capacity, depression, and personality changes ▶Fatigue,Seizures Chronic hypocalcemia - dermatologic manifestations: ▶Coarse hair,Brittle nails ▶Psoriasis,Dry skin ▶Chronic pruritus ▶Poor dentition
- 14. ▶ Hair may appear coarse, and alopecia may be present. ▶ In chronic hypocalcemia - dental caries,enamel hypoplasia. ▶ Eye examination-subcapsular cataract or papilledema ▶ Patient may appear confused, disoriented, Irritabile ▶ Hallucinations, dementia, and seizures may occur. ▶On R/S-wheezes , laryngeal stridor ▶ On CVS- bradycardia, tachycardia, S3 , signs of HF. PHYSICAL EXAMINATION
- 15. ▶Chvostek sign - tapping the skin over the facial nerve about 2 cm anterior to the external auditory meatus. ▶Ipsilateral contraction of the facial muscles is a positive sign. ▶Depending on the ca level, a graded response will occur: twitching first at the angle of the mouth, then by nose, eye and the facial muscles. ▶ 10% of the population will have a positive Chvostek sign in the absence of hypocalcemia so test is not diagnostic
- 16. ▶ Trousseau sign- placing a blood pressure cuff on the patient’s arm and inflating to 20 mm Hg above SBP for 3-5 minutes. ▶flexion of wrist and MCP joints ,extension of IP joints and adduction of the thumb (carpal spasm). ▶The Trousseau sign is more specific than the Chvostek sign Extra pyramidal symptom : ▶Choreoathetosis ,Parkinsonism,Hemiballism
- 18. CAUSES and Diagnostic Approach LOW PARATHYROID HORMONE LEVEL HIGH PARATHYROID HORMONE LEVEL PARATHYROID • AGENESIS-digeorge •DESTRUCTION surgical radiation infiltration autoimmune •HYPOFUNCTION-mg,CaSR •VIT D related Deficiency Renal insufficiency Resistance •PTH horm resistance syndromes •DRUGS Chelators,biphosphanates Miscellaneous Acute pancreatitis Acute rhabdomyolisis Hungry bone Osteoblastic metastasis
- 19. ▶On X-RAY, rickets or osteomalacia may present with the pathognomonic Looser zones, better observed in the pubic ramus, upper femoral bone, and ribs. ▶CT scans of head may show basal ganglia calcification (extrapyramidal neurologic symptoms )
- 20. ▶Mild to Moderate Hypocalcemia,asymptomatic needs only ca supplement ▶IV replacement is recommended in symptomatic or severe hypocalcemia. ▶Doses of 100-300 mg of elemental ca in 50-100 mL of 5% D should be given over 5-10 minutes. ▶10 mL of calcium gluconate contains 90 mg elemental ca ▶10 mL of calcium chloride contains 272 mg elemental ca Treatment
- 21. ▶Measure serum calcium every 4-6 hours to maintain at levels of 8-9 mg/dL. ▶Start oral calcium and vitamin D treatment early ▶oral calcium supplements must be given between meals otherwise, they will act as phosphate binders ▶ Vit D deficiency - vitamin D supplementation (50,000 U, 2–3 times per week for several months) ▶ Vit D deficiency due to malabsorption- higher doses (100,000 U/d or more).