Journal club PROSTHODONTICS
•Télécharger en tant que PPTX, PDF•
10 j'aime•1,932 vues

COMPARISON OF CONVENTIONAL CAD CAM AND 3D PRINTING IN MANUFACTURE OF DIFFERENT PROSTHESIS

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Journal club PROSTHODONTICS
Similaire à Journal club PROSTHODONTICS (20)
Plus de NAMITHA ANAND
Plus de NAMITHA ANAND (20)
Dernier
Dernier (20)
Journal club PROSTHODONTICS
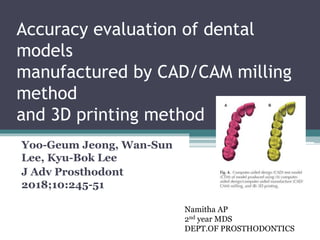
- 1. Accuracy evaluation of dental models manufactured by CAD/CAM milling method and 3D printing method Yoo-Geum Jeong, Wan-Sun Lee, Kyu-Bok Lee J Adv Prosthodont 2018;10:245-51 Namitha AP 2nd year MDS DEPT.OF PROSTHODONTICS
- 2. CONTENTS • INTRODUCTION • AIM • MATERIALS AND METHODS • RESULTS • DISCUSSION • RELATED ARTICLES • CONCLUSION • REFERENCES
- 3. INTRODUCTION Taking a dental impression TRADITIONAL METHODS Affected by skill level and technique of practitioner DIGITAL METHODS CAD CAM MILLING 3D PRINTING
- 4. DISADVANTAGES OF CAD CAM Material wastage high maintenance cost of the equipment time loss ADVANTAGES OF 3D PRINTING Minimum amount of material Maximum number of products
- 5. AIM • To evaluate the accuracy of a model made using the computer-aided design/computer-aided manufacture (CAD/CAM) milling method and 3D printing method and to confirm its applicability as a work model for dental prosthesis production
- 6. MATERIALS AND METHODS • scanned using an oral scanner natural tooth model (ANA-4,Frasaco, Germany) • From obtained scan data CAD Reference Model(CRM) • 10 each using milling method and 3D printing method Total 20 models • CAD test model was formed 20 models were then scanned using a desktop scanner
- 7. Synthetic resin Denture model Negative model using dental silicone Model cast using hard plaster reference STL file CAD Reference Model(CRM) Intra oral scanner Trios (3Shape, Copenhagen, Denmark). 10 Milling Models with PMMA blocks 10 3D Printed models Desktop scanner
- 10. • Kept as control Reference STL files • Kept as test groups Test STL files Each test STL file was superimposed on the reference STL file using specialized software (Geomagic Control X, 2017.0.3, 3D Systems, Cary, NC, USA). test STL file was converted into point cloud data CAD-reference- model (CRM), surface date, CAD- test-model (CTM), and the point cloud data,were initially aligned rearranged to the best fit alignment. point cloud data was projected onto the surface of the CRM data.
- 11. The distances between surface data and all points were converted to root mean square (RMS) values. The RMS is a general method to assess the mean value of errors, by directly comparing two data groups with an identical coordinate system. The accuracy of a corresponding data group can be calculated using a single scale. A higher calculated RMS value indicated a large error, i.e., the difference in the attributes between reference and measurement data. The RMS is typically used as a criterion to measure the similarity of two sets of N-dimensional vector sets after optimal superimposition.
- 12. Unnecessary and inaccurate parts of the 3D shape data of all models were eliminated.The superimposition results were illustrated as a color difference map Max +100µm Min -100µm Effective range(green) -30 μm to +30 μm.
- 13. 42 assigned points Incisal angle of incisors(4) Cusp of the molars(10) Undercut in the facial aspect(7) Undercut in the lingal aspect(7) Fossa/pit of molars(10) Lingual fossa of incisors(3) Tip of cusp of canine(1) For the location of these points, the divergences in the x-, y-, and z-axis to each reference and the test data were measured.15
- 14. Results
- 15. results of the accuracy assessment of the manufacturing methods, which was conducted using test software
- 16. the two models were measured by using the fixed measuring points (e.g. cusp tip and fossa) in order to evaluate the clinical correlation of the discrepancies observed in between the models through RMS methods. results of the superimposition for 10 specimens in each group are
- 18. Discussion Data using measuring points Milling 5 axis maching equipment 152 ± 52 μm 3D printing SLA 3D printer with 16 µm layer 52 ± 9 μm • Showed statistical significance between the two manufacturing methods • milling method presented smaller difference in the fossa compared to 3D printing method. • This is thought to be the outcome of the crushed materials in the pit in 3D printing method • whereas the deepest region (pit) of the fossa was manufactured by the milling bur in milling method. 3D printing method was significantly more accurate than the milling method (P = .001).
- 19. color difference maps of two models were analyzed using inspection software • compared to group B, group A showed red and blue areas in the occlusal surface, interdental space, and gingival sulcus. • inferior to 3D printing, in terms of the reproducibility ofthese regions (i.e., the interdental space, gingival sulcus, and occlusal surface).
- 20. CRITICAL EVALUATION • the minimumNthickness of the bur was 1 mm in the milling process, which limited the accurate reproduction of shapes that were smaller than 1 mm. • bur of less than 1 mm could not be used since PMMA resin was used as the milling material to produce the model. Since burs less than 1 mm (e.g., 0.6mm) are easily heated, this would have caused the resin to be melted and adsorbed onto the bur, fracturing the bur in the process. • data locations for the manufacture of a working model were selected on the CAM software before machining so that two models were arranged per single block. Although this arrangement was chosen to prevent the fracture of the bur and reduce the number of machining processes, it could have also affected the accuracy of the model.
- 21. CONCLUSION • The current study demonstrated that models manufactured by the 3D printing method were more accurate than those manufactured by the milling method, within the limitations of the study. However, currently, it is still challenging to apply the models manufactured by milling and 3D printing method as working models for dental prostheses manufacture.
- 22. RELATED ARTICLES
- 23. Accuracy of dental models fabricated by CAD/CAM milling method and 3D printing method. Wook-Tae Kim. J Oral Res 2018; 7(4):127-133.
- 24. Aim of the study to evaluate the accuracy of a dental model fabricated using the CAD/CAM milling method and the 3D printing method.
- 25. Materials and methods Digitisation of master model using intra oral scanner manufacturing of working models (milling model, Multi- jet printing model and Color-jet printing model) by using the scan data of the master model e digitization of the working model by using a laboratory scanner, the superimposition of the digital data of the master model and working models using inspection software 3-dimensional analysis.
- 26. Ten measurements per group were done by one practitioner
- 27. Results
- 29. Conclusion • Dental models manufactured by the CAD/CAM milling method presented superior accuracy over the models manufactured by the 3D printing method. Therefore, the use of optimized CAD software and appropriate materials is crucial for the fabrication accuracy of dental models.
- 30. Evaluation of internal fit of interim crown fabricated with CAD/CAM milling and 3D printing system Wan-Sun Lee Du-Hyeong Lee Kyu-Bok Lee J Adv Prosthodont 2017;9:265-70
- 31. Aim of the study to evaluate the internal fit of the crown manufactured by CAD/CAM milling method and 3D printing method.
- 32. Materials and methods The master model was fabricated with stainless steel by using CNC machine and the work model was created from the vinyl- polysiloxane impression After scanning the working model, the design software is used to design the crown.
- 33. The saved STL file is used on the CAD/CAM milling method and two types of 3D printing method to produce 10 interim crowns per group.
- 34. Internal discrepancy measurement uses the silicon replica method and the measured data are analyzed with One-way ANOVA to verify the statistic significance.
- 35. The discrepancy means (standard deviation) of the 3 groups are 171.6 (97.4) μm for the crown manufactured by the milling system and 149.1 (65.9) and 91.1 (36.4) μm, respectively, for the crowns manufactured with the two types of 3D printing system. There was a statistically significant difference and the 3D printing system group showed more outstanding value than the milling system group.
- 36. Results
- 37. Conclusion • The marginal and internal fit of the interim restoration has more outstanding 3D printing method than the CAD/CAM milling method. Therefore, the 3D printing method is considered as applicable for not only the interim restoration production, but also in the dental prosthesis production with a higher level of completion.
- 38. CAD-CAM milled versus rapidly prototyped (3D-printed) complete dentures: An in vitro evaluation of trueness Nicole Kalberer, Albert Mehl, Martin Schimmel, Frauke Müller, Murali Srinivasan, (J Prosthet Dent 2018)
- 39. Aim of the study to compare the differences in trueness between the CAD-CAM milled and 3D-printed complete dentures.
- 40. Materials and methods third scan (after the wet-dry cycle) was then made after 21 days, during which the complete dentures were maintained in the artificial saliva solution during the day and stored dry at night. immersed in an artificial saliva solution for a period of 21 days, followed by a second scan (after immersion in saliva). intaglio surfaces of the fabricated complete dentures were scanned at baseline using a laboratory scanner. Two groups of identical maxillary complete dentures were fabricated 3D-printed denture group (3DPD) (n=10) milled denture group (MDG) (n=10)
- 41. • A purpose-built 3D comparison software program was used to analyze the differences in the trueness of the complete dentures. The analyses were performed • Independent t tests, ANOVA, and post hoc tests were used for statistical analyses (a=.05). Entire intaglio surface Mid palatal raphe Vestibular flange Anterior ridge Posterior crest Palatal vault Posterior palatal seal area tuberosity
- 43. Results The trueness of the milled prostheses was significantly better than that of the rapid prototyping group with regard to the entire intaglio surface (P<.001), posterior crest (P<.001), palatal vault (P<.001), posterior palatal seal area (P<.001), tuberosity (P<.001), anterior ridge (baseline: P<.001; after immersion in saliva: P=.001; after the wet-dry cycle: P=.011), vestibular flange (P<.001), and mid-palatal raphae (P<.001).
- 45. Conclusion • The CAD-CAM, milled complete dentures, under the present manufacturing standards, were superior to the rapidly prototyped complete dentures in terms of trueness of the intaglio surfaces. • Further research is needed on the biomechanical, clinical, and patient-centered outcome measures to determine the true superiority of one technique over the other with regard to fabricating complete dentures by CAD-CAM techniques.
- 46. Comparing accuracy of denture bases fabricated by injection molding, CAD/CAM milling, and rapid prototyping method Suji Lee Seoung-Jin Hong Janghyun Paek Ahran Pae Kung-Rock Kwon Kwantae Noh
- 47. Aim of the study • . The accuracy of denture bases was compared among injection molding, milling, and rapid prototyping (RP) fabricating method
- 48. The maxillary edentulous master cast was fabricated and round shaped four notches were formed. The cast was duplicated to ten casts and scanned. Denture bases were milled from a pre-polymerized block in the milling method. In the RP method, denture bases were printed and post-cured.
- 49. In the injection molding method, designed denture bases were milled from a wax block and fabricated using SR Ivocap injection system.
- 50. The intaglio surface of the base was scanned and surface matching software was used to measure inaccuracy
- 51. Measurements were performed between four notches and two points in the mid-palatal suture to evaluate inaccuracy. The palatine rugae resolution was evaluated.
- 52. Measurements were performed between two points in the mid-palatal suture to evaluate inaccuracy. The palatine rugae resolution was evaluated.
- 54. Results No statistically significant differences in distances among four notches (P>.05). The accuracy of the injection molding method was lower than those of the other methods in two points of the mid- palatal suture significantly (P<.05). The degree of palatine rugae resolution was significantly higher in the injection molding method than that in other methods (P<.05).
- 56. Conclusion • Overall accuracy of the denture base is higher in milling and RP method than the injection molding method. The degree of fine reproducibility is higher in the injection molding method than the milling or RP method.
- 57. REFERENCES
- 58. THANK YOU!!!
Notes de l'éditeur
- pouring a semiflexible material into a dental impression tray, which was then solidified. This procedure were inconvenient to patients