
Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à heart cardiac cycle
Similaire à heart cardiac cycle (20)
Dernier
Dernier (20)
heart cardiac cycle
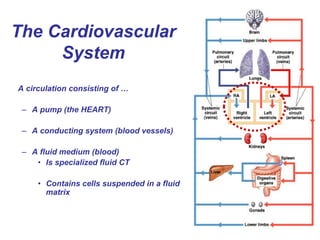
- 1. The Cardiovascular System A circulation consisting of … – A pump (the HEART) – A conducting system (blood vessels) – A fluid medium (blood) • Is specialized fluid CT • Contains cells suspended in a fluid matrix
- 2. Important BASIC “RULES” of the CV system: This is independent of the OXYGEN content of the blood i.e the amount of HbO2. 1. By convention, arteries carry blood AWAY from the heart and VEINS towards it.
- 3. 2. The normal pattern of blood flow through the vasculature is …. • From the HEART → TISSUES in ARTERIES • “CONDUCTIING VESSELS” • Distribution of nutrients etc. in CAPILLARIES • “EXCHANGING VESSELS” • From the TISSUES → HEART in VEINS • “CAPACITANCE VESSELS” An EXCEPTION to this pattern is called a PORTAL CIRCULATION.
- 4. The HUMAN heart has 4 interconnected chambers. 3. BLOOD FLOW through those chambers is UNIDIRECTIONAL.
- 5. The HEART VALVES ensure unidirectional flow. 2 AV valves: - Lt. AV (bicuspid/mitral) - Rt. AV (tricuspid) 2 Semilunar valves: - aortic valve - pulmonary valve
- 6. Thus, the normal adult pattern of blood flow would be …
- 8. Right atrium Right ventricle Papillary muscle Chordae tendineae Septum AV valve structure
- 10. When pressure is greater “UPSTREAM, it opens. When pressure is greater “DOWNSTREAM” , it closes. It does not open in the opposite direction; that is, it is a 0NE-WAY VALVE. 4. All heart valves are PASSIVE.
- 11. “DOWNSTREAM” “UPSTREAM” When pressure is greater “UPSTREAM, the valve is OPEN. When pressure is greater “DOWNSTREAM” , the valves is CLOSED. It does not open in the opposite direction; that is, it is a 0NE-WAY VALVE.
- 12. What must the pressure relationships between chambers or between chambers and draining vessels be, in each of the following diagrams?
- 13. 4. In an adult, blood CANNOT flow from the right side of the heart to the left side without LEAVING the heart. The RIGHT VENTRICLE pumps blood through the PULMONARY CIRCUIT and the LEFT VENTRICLE pumps blood through the SYSTEMIC CIRCUIT.
- 14. 5. BLOOD “flows” through the vasculature DOWN a PRESSURE GRADIENT created by the contraction of the heart. We call this pressure the BLOOD PRESSURE or more precisely the MEAN ARTERIAL PRESSURE (MAP).
- 15. 6. MAP is the REGULATED VARIABLE in the CARDIAC REFLEXES. The GOAL of the CV system is to MAINTAIN MAP, i.e. maintain what causes the blood to flow.
- 17. The HEART is located in the THORACIC CAVITY. It is found in a non-delineated space MEDIAL to the LUNGS called the MEDIASTINUM.
- 18. Its BASE is located SUPERIORLY and its APEX, INFERIORLY. It is ROTATED counterclock-wise so as to lie on its RIGHT SIDE. Base Apex
- 19. The BASE of the heart lies at the level of the 2nd intercostal space at midline. The APEX lies at the level of the 5th intercostal space about 2.5-3” to the LEFT of midline.
- 20. The heart lies in the PERICARDIAL CAVITY, surrounded by the a SEROUS MEMBRANE called the PERICARDIUM.
- 21. Serous membranes consist of TWO epithelial “membranes” facing each other i.e. are DOUBLE layered and contain a fluid filled space.
- 22. A section of the heart showing its three layers: epicardium, myocardium, and endocardium Myocardium Endocardium Epicardium Parietal Pericardium Dense fibrous layer Areolar tissue Mesothelium Mesothelium Areolar tissue Connective tissues Pericardial space (contains serous fluid) Muscular wall of the heart consisting primarily of cardiac muscle cells Areolar tissue Covers the inner surfaces of the heart Endothelium Covers the outer surface of the heart; also called the visceral pericardium The serous membrane that forms the outer wall of the pericardial cavity; it and a dense fibrous layer form the pericardial sac surrounding the heart The OUTER membrane is called the PARIETAL PERICARDIUM, the INNER membrane the VISCERAL PERICARDIUM and the space between them the PERICARDIAL SPACE.
- 23. The pericardium STABILIZES the position of the heart and associated vessels within the mediastinum. The SEROUS FLUID in the pericardial space LUBRICATES and eliminates FRICTION between the heart and adjacent tissues as the heart beats.
- 24. Externally, the CORONARY SULCUS marks the separation between the atria and ventricles.
- 25. Similarly, the ANTERIOR & POSTERIOR INTERVENTRICULAR SULCI indicate the location of the interventricular septum.
- 26. Commonly, significant accumulations of WAT (structural fat) are found in these sulci, … Mesothelium (visceral pericardium)
- 27. … as are the major cardiac arteries and veins.
- 28. Most of the heart consists of CARDIAC MUSCLE. This muscular component is called the MYOCARDIUM. It is made up of cardiac muscle cells or CARDIOMYOCYTES.
- 29. The ORIENTATION of the cardiac muscle cells means that the contracts with a “wringing” motion from APEX to BASE.
- 30. Fibrous CT (fibrous trigone) anchors the valves and almost completely separates the atrial myocardium from the ventricular myocardium.
- 31. The internal surfaces of the heart are lined by a simple squamous epithelium called the ENDOCARDIUM. This is continuous with the ENDOTHELIUM that lines the blood vessels.
- 32. A section of the heart showing its three layers: epicardium, myocardium, and endocardium Myocardium Endocardium Epicardium Parietal Pericardium Dense fibrous layer Areolar tissue Mesothelium Mesothelium Areolar tissue Connective tissues Pericardial cavity (contains serous fluid) Muscular wall of the heart consisting primarily of cardiac muscle cells Areolar tissue Covers the inner surfaces of the heart Endothelium Covers the outer surface of the heart; also called the visceral pericardium The serous membrane that forms the outer wall of the pericardial cavity; it and a dense fibrous layer form the pericardial sac surrounding the heart Thus, the point of a pin entering the pericardial cavity from the outside ….
- 34. 4. The heart relies completely on AEROBIC RESPIRATION for its energy, and is unable to pump sufficiently in an ISCHEMIC (oxygen-deprived) environment. The heart, as a muscle, pumps continuously throughout life and is adapted to be highly resistant to fatigue. 2. Cardiomyocytes contain large numbers of mitochondria, enabling continuous aerobic respiration and production of ATP. 3. Cardiac muscle also contains MYOGLOBIN, an oxygen-storing protein. 1. Cardiac muscle has an extensive supply from the CORONARY ARTERIES that provide nutrients and oxygen.
- 35. The CORONARY CIRCULATION is the circulation to and from the heart itself. The largest elements of this circulation are visible on the surface of the heart, deep to the epicardium.
- 36. The CORONARY ARTERIES are the initial branches of the AORTA. They originate practically behind the cusps of the aortic valve!
- 37. The heart is supplied with blood from the LEFT & RIGHT CORONARY ARTERIES.
- 38. Branches of these arteries penetrate the myocardium.
- 39. Consequently, only a small portion of the cardiac vasculature is visible on the surface of the heart.
- 40. Generally speaking, the left CA supplies the LEFT side of the heart and the right CA the RIGHT.
- 41. The CORONARY SINUS receives most of the venous return from the heart.
- 42. In a cardiac bypass, blood flow is restored by “detouring” around a blockage in a coronary artery.
- 43. In the fetal circulation, blood is pumped by the heart TO the TISSUES and FROM the TISSUES back to the heart. However, the PULMONARY circuit is essentially inoperative since ….. THE FETAL CIRCULATION
- 44. …..the fetus obtains oxygen and nutrients from the mother through the PLACENTA via the UMBILICAL CORD. There is no direct contact between fetal and maternal blood.
- 45. Umbilical cord An UMBILICAL/PLACENTAL VEIN delivers oxygenated blood TO the fetus and 2 UMBILICAL ARTERIES return venous blood FROM the fetus to the placenta.
- 46. On entering the fetus, the umbilical vein BYPASSES the fetal liver via the DUCTUS VENOSUS. It then joins the fetal INFERIOR VENA CAVA. Thus the oxygenated blood from the placenta MIXES with fetal venous, deoxygenated blood.
- 47. This is the reason that the higher affinity of HbF for oxygen is advantagous! PO2 umbilical artery = 35 mm Hg PO2 adult arterial blood = 100 mm Hg
- 48. This “mixed” blood enters the fetal heart via the RIGHT ATRIUM. A small portion of it passes to the RIGHT VENTRICLE and completes the PULMONARY CIRCUIT, re-entering the heart via the LEFT ATRIUM.
- 49. Alternatively, rather than flowing to the LUNGS via the PULMONARY TRUNK, blood may flow DIRECTLY into the fetal AORTA via the DUCTUS ARTERIOSUS.
- 50. ….. OR, blood can pass directly from the RIGHT ATRIUM to the LEFT ATRIUM via the FORAMEN OVALE, located in the interatrial septum.
- 51. However it gets there, blood from the AORTA is distributed to the fetal tissues. It RETURNS to the PLACENTA via the 2 UMBILICAL ARTERIES.
- 54. Most of the heart consists of CARDIAC MUSCLE. This muscular component is called the MYOCARDIUM.
- 55. Striated muscle Unstriated muscle Skeletal muscle Cardiac muscle Smooth muscle Voluntary muscle Involuntary muscle ANATOMICALLY, cardiac muscle is like skeletal muscle. PHYSIOLOGICALLY, it is smooth muscle.
- 56. Cardiac muscle is STRIATED. • Contains SARCOMERES • Contains ACTIN, MYOSIN and TROPONIN • Contraction explained by the SLIDING FILAMENT MODEL • Excitation/contraction coupling via Ca++
- 57. Cardiac muscle cells are interconnected via INTERCALATED DISCS.
- 58. GAP JUNCTIONS located in the INTERCALATED DISCS cause the myocardium to function as a SYNCYTIUM.
- 59. Striated muscle Unstriated muscle Skeletal muscle Cardiac muscle Smooth muscle Voluntary muscle Involuntary muscle ANATOMICALLY, cardiac muscle is like skeletal muscle. PHYSIOLOGICALLY, it is smooth muscle.
- 60. Cardiac muscle cells are INVOLUNTARY, i.e. their CONTRACTION is regulated …. • INTRINSICALLY by PACEMAKER activity
- 61. Cardiac muscle cells are INVOLUNTARY, i.e. their CONTRACTION is regulated …. • EXTRINSICALLY by the ANS and ENDOCRINE SYSTEMS
- 62. Cardiac muscle is an EXCITABLE tissue!!! It consists of 2 populations of excitable cells – -Contractile cardiomyocytes -Pacemaker cardiomyocytes
- 63. Contractile cells make up the bulk of the myocardium. They are specialized for contraction.
- 64. Pacemaker cells are contained within the INTRINSIC CONDUCTION SYSTEM. They are specialized for conduction, and are responsible for the COORDINATED contraction of the contractile cells.
- 65. PACEMAKER action potentials initiate the action potentials in CONTRACTILE cells, which result in their CONTRACTION. They are thus referred to as PACEMAKER POTENTIALS.
- 66. Since the pacemaker cardiomyocytes are linked by GAP JUNCTIONS to the contractile cardiomyocytes … …when the pacemaker cells depolarize, so do the contractile cells, AT THE SAME TIME AND RATE! Thus the INHERENT pacemaker activity of these cardiomyocytes determines the INTRINSIC CONTRACTILE RATE OF THE HEART!
- 67. 2. AT ANY MOMENT IN TIME the membrane potential is produced by the WEIGHTED AVERAGE of all the ions in DISEQUILIBRIUM to which it is PERMEABLE. 1. PACEMAKER CELLS have an inherently UNSTABLE membrane potential that DEPOLARIZES over time. This is called a PACEMAKER or PREPOTENTIAL. The pacemaker potential gradually becomes less negative until it reaches THRESHOLD and triggers an ACTION POTENTIAL.
- 68. 3. DURING THE PREPOTENTIAL the membrane’s permeability to THREE IONS- Na+, K+ and Ca++ - changes AND SO DOES THE VALUE OF THE MEMBRANE POTENTIAL. 1. K+ permeability DECREASES throughout. 2. Na+ permeability INCREASES slightly. NET EFFECT: the membrane potential “drifts” towards a more positive value.
- 69. 3. As membrane potential approaches -50 mV, Ca++ (T) channels open. 4. As membrane potential approaches -40 mV Ca++ (L) channels open. This brings the membrane to threshold. The L-type channels open EXPLOSIVELY and the membrane rapidly DEPOLARIZES.
- 70. N.B. UNLIKE neurons, depolarization in pacemaker cardiomyocytes is due to an influx of Ca++ NOT Na+!
- 71. 4. At maximum depolarization, the L-type channels CLOSE and the K+ channels OPEN, initiating REPOLARIZATION.
- 72. The pacemaker cells are arranged in an interconnected pathway called the INTRINSIC CONDUCTION SYSTEM. SA node
- 73. Each population of pacemaker cells in the intrinsic conduction system has its own inherent rate of depolarization. • SA node – 100 times/minute • AV node – 40-60 times/minute • Purkinje fibers – 30-40 times/minute
- 74. The fastest depolarizing element in the conduction becomes THE pacemaker for the entire myocardium. The pacemaker activity of the slower depolarizing elements is inhibited. This is called OVERDRIVE SUPPRESSION.
- 75. If the fastest group of cells is inhibited, the NEXT fastest group becomes THE pacemaker!
- 76. If the “linkage” between the SA node and the pacemaker cells in the ventricles is broken, atria and ventricular myocardia beat independently. This is called a HEART BLOCK.
- 77. An ECTOPIC FOCUS is a group of cells that transiently depolarizes more rapidly than the normal pacemaker. In a normal, healthy heart this is usually SELF-LIMITING. Causes include: fatigue, caffeine, ANS irregularities
- 78. Transmission of the cardiac impulse through the heart, showing the time of appearance (in fractions of a second after initial appearance at the sinoatrial node) in different parts of the heart. © 2005 Elsevier Although all regions of the myocardium are functionally united by this system….
- 79. … passage of the beat through the fibrous trigone DELAYS transmission of the beat by about 200 msec. Thus the atria depolarize and contract about 200 msec. BEFORE the ventricular myocardium.
- 80. Pacemaker cell Contractile cell Action potentials in CONTRACTILE cardiomyocytes is characterized by a prolonged PLATEAU PHASE.
- 81. Contractile cardiomyocyte • Prolonged Ca++ INFLUX following depolarization produces a broad PLATEAU phase. • These voltage-gated channels are termed L- type calcium channels (L for Long lasting)
- 82. Action potentials & contraction in skeletal muscle
- 83. The difference in duration of the action potential (10 msec.) and contraction (100 msec.) in skeletal muscle permits SUMMATION, TETANUS and eventual FATIGUE.
- 84. Action potentials & contraction in contractile cardiomyocytes In cardiac muscle the duration of the action potential extends through most of the contraction.
- 85. Consequently, SUMMATION and its consequences cannot occur in cardiac muscle.
- 86. Of course, all this electrical activity IS measurable. The ECG (EKG) represents the SUMMATION of all of the electrical activity associated with one “heartbeat”.
- 87. Electrodes placed on the skin detect and amplify the minute electrical activity occurring in the heart.
- 88. – P wave • atrial depolarization – QRS complex • vent. depolarization – T wave • vent. repolarization – PR interval • AV nodal delay – QT segment • ventricular systole – TQ interval • ventricular diastole A normal ECG (EKG)
- 89. The Cardiac Cycle: Systole and diastole
- 90. The Cardiac Cycle Heart rate = 72 bpm - 72 cardiac cycles/minute - each cardiac cycle = 0.83 seconds - or about 800 msec.
- 91. • ELECTRICAL ACTIVITY precedes CONTRACTION. • Atrial SYTOLE lasts about 100 msec. • Ventricular SYSTOLE lasts about 300 msec. • At this rate of contraction, the ENTIRE heart is in SIMULTANEOUS DIASTOLE for the last half of the cycle.
- 92. A CARDIAC CYCLE consists of one set of atrial and ventricular systoles and diastoles. Since both “sides” of the heart and doing the same thing at the same time, we can deal with a “half heart”. By convention, this is the LEFT side or SYSTEMIC PUMP. By convention, one assumes a normal heart “at rest”.
- 93. Under these circumstances the HEAERT RATE is about 72 beat/min (bpm). - 72 cardiac cycles/minute - each cardiac cycle = 0.83 seconds - or about 800 msec. • ELECTRICAL ACTIVITY precedes CONTRACTION. • Atrial SYTOLE lasts about 100 msec. • Ventricular SYSTOLE lasts about 300 msec. • At this rate of contraction, the ENTIRE heart is in SIMULTANEOUS DIASTOLE for the last half of the cycle.
- 94. Wiggers diagram
- 95. The cardiac cycle begins with VENTRICULAR FILLING. What is the valvular configuration?
- 96. Because the pressure in the atrium is greater than the pressure in the ventricle, the AV valves are OPEN. Because the pressure in the aorta is greater than the pressure in the ventricle, the aortic valve is CLOSED.
- 97. The RATE of ventricular filling is PASSIVE and NON-UNIFORM. Initial filling is rapid and then slows.
- 98. At the end of ATRIAL DIASTOLE, the SA node fires and the atria depolarize and CONTRACT.
- 99. Right atrium Right ventricle Passive Left ventricle Left atrium Atrial contractionVentricular filling A B Atrial contraction
- 100. This adds a small, additional amount of blood to the ventricle (~ 15 mls). This is the END DIASTOLIC VOLUME (EDV) EDV = volume of blood in ventricle at end of (ATRIAL) diastole (~ 130 mls)
- 101. About 100 msec. later, the VENTRICLES depolarize and CONTRACT.
- 102. The contraction of the ventricles raises the ventricular pressure ABOVE the atrial pressure, and the AV VALVES CLOSE.
- 103. The 1st HEART SOUNDS occur as the AV VALVES close.
- 104. However, the pressure in the ventricles is still LOWER than that in the aorta, so the aortic valves remain closed. ISOVOLUMETRIC VENTRICULAR CONTRACTION
- 105. As the pressure in the ventricles exceeds that in the aorta, the AORTIC VALVE OPENS and blood enters the aorta. VENTRICULAR EJECTION Since the pressure in the ventricle is still greater than the pressure in the atrium, the AV valve remains closed.
- 106. The volume of blood remaining in the ventricle AFTER ejection i.e. after ventricular systole is called the END SYSTOLIC VOLUME. The volume of blood ejected into the aorta is the STROKE VOLUME.
- 107. – EDV = volume of blood in ventricle at end of diastole (~ 130 mls) – ESV = volume of blood in ventricle at end of systole (~ 65 mls) – SV = volume of blood ejected from heart each cycle SV = EDV – ESV
- 108. If the EDV = 135 mls and the SV = 65 mls, then the EJECTION FRACTION = 65/135 = 48% This can also be expressed as a fraction (the EJECTION FRACTION).
- 109. As the ventricles begin to relax into diastole, the pressure falls BELOW the pressure in the aorta and the AORTIC VALVES CLOSE.
- 110. The 2nd HEART SOUNDS occur as the SEMILUNAR VALVES close.
- 111. The pressure in the ventricles is still greater than the pressure in the atria, so the AV valves still remain CLOSED. The heart is thus in simultaneous diastole with ALL VALVES CLOSED. ISOVOLUMETRIC VENTRICULAR RELAXATION
- 112. As the pressure in the ventricles rapidly declines during diastole, it falls BELOW that in the ATRIA and the AV VALVES OPEN. Since the pressure in the atria is BELOW that in the aorta, the aortic valve remains closed. VENTRICULAR FILLING begins as the CARDIAC CYCLE repeats itself.
- 114. Fetal Hb, with its HIGHER AFFINITY O2, compensates for the lower PO2.
- 115. Cardiac Muscle Cells/cardiomyocytes • Characteristics of Cardiac Muscle Cells – Small size – Single, central nucleus – Branching interconnections between cells
- 116. Orientation of contractile cardiac fibers Cardiomyocytes spiral superiorly, from the apex to the base.
- 117. The PULMONARY circulation is a low pressure system, the SYSTEMIC circulation a high pressure system. Whether WITHIN the heart and in BOTH the SYSTEMIC and PULMONARY circulations, BLOOD ALWAYS FLOWS DOWN A PRESSURE GRADIENT.