Laryngeal Dystonia: Causes, Symptoms and Treatment
•Télécharger en tant que PPTX, PDF•
7 j'aime•2,452 vues

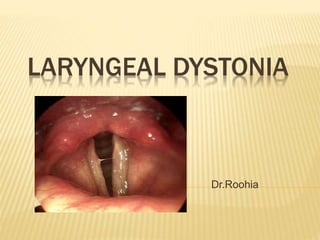
Laryngeal dystonia, also known as spasmodic dysphonia, is a focal dystonia that affects the muscles of the larynx involved in speech production. It causes involuntary spasms of the vocal folds during speech, resulting in interruptions in phonation and changes to the voice quality. The spasms are usually task-specific, only occurring during voluntary speech and not other vocal behaviors like laughing or crying. There are different subtypes depending on whether the spasms cause hyperadduction or incomplete adduction of the vocal folds. Neurologically, it is thought to involve alterations in connectivity between the laryngeal motor cortex and brainstem nuclei responsible for phonation. Treatment involves voice therapy and in some

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (18)
Similaire à Laryngeal Dystonia: Causes, Symptoms and Treatment
Similaire à Laryngeal Dystonia: Causes, Symptoms and Treatment (20)
Plus de Md Roohia
Plus de Md Roohia (20)
Dernier
Dernier (20)
Laryngeal Dystonia: Causes, Symptoms and Treatment
- 2. DYSTONIA Dystonias are a group of movement disorders that are characterized by involuntary, action- induced counterproductive muscle contraction. Laryngeal dystonia(Spasmodic dysphonia (SD): is a focal dystonia affecting the neural control of the laryngeal musculature for speech production. Spastic aphonia, spastic dysphonia, phonic laryngeal spasm, coordinated laryngeal spasms, mogiphonia, and laryngeal stuttering.
- 3. REQUIREMENTS FOR SPEECH PRODUCTION Respiration Phonation Articulation Resonance
- 4. WHAT IS REQUIRED FOR SOUND PRODUCTION? Sound production requires two things: Power/energy source Vibrating element When it comes to speech production, the power source is air that comes from the lungs and the vibration occurs in the vocal cords
- 5. RESPIRATION Also known as breathing Two phases: Inhalation Also known as inspiration Occurs when diaphragm lowers, which causes increased volume/space in thoracic cavity. This results in negative pressure in the lungs compared to the atmospheric pressure outside the lungs; therefore, air rushes from outside the body into the oral and nasal cavities, down the trachea, and into the lungs. Exhalation Also known as expiration The decrease in the volume/space of thoracic cavity after inhalation results in positive pressure in the lungs. If the airway is open, air will rush out of the lungs (up the trachea and out the oral and nasal cavities) in order to equalize the outside and inside pressure.
- 6. PHONATION The act of phonation occurs in the larynx, where the vocal cords are housed The larynx is also called the “voice box”
- 7. PHONATION When air from the lungs is forced through closed vocal cords, the vocal cords vibrate and phonation occurs The pitch of sounds produced in the larynx is dependent upon the tension of the vocal cords Elongation and tension of the cords results in faster vibration = higher frequency/pitch Shortening and relaxation of the cords results in slower vibration = lower frequency/pitch Fundamental frequency of male voice=130 Hz Fundamental frequency of female voice=220 Hz The loudness of sounds produced in the larynx is dependent upon the speed of air flowing through the glottis (space between the cords). The air speed is greatest when the pressure build-up below the vocal cords (subglottal pressure) is high
- 8. ANATOMY: LARYNGEAL CARTILAGE The Larynx is composed of: Cartilages (6) Single cartilages: Epiglottis, thyroid, cricoid Paired cartilages: Arytenoid, corniculate and cuneiform Muscles & Ligaments Support and connect the cartilages of the larynx Form the vocal cords
- 11. ANATOMY: LARYNGEAL MOTION Abduction of vocal ligament
- 12. ANATOMY: LARYNGEAL MOTION Adduction of vocal ligament
- 13. ANATOMY: LARYNGEAL MOTION Tension of vocal ligament
- 14. VOCAL CORDS Also referred to as vocal folds Housed within the larynx Attached anteriorly to the thyroid cartilage and posteriorly to the arytenoid cartilages Closed when we swallow to protect our airway Open when we are breathing in order to allow air in/out of lungs Vibrate open and closed during phonation
- 17. THE PERIODS OF VOCAL FOLD CONTACT AND LACK OF CONTACT IN ONE VIBRATORY CYCLE Phase Description Closing The vocal folds begin to close rapidly from their lower margin Closed The medial edges of the vocal folds are in full contact Opening The vocal folds begin to separate from their lower margin and gradually peel apart. The superior margin remains in contact until the end of this phase Open The vocal folds are separated, the longest part of a normal vibratory cycle
- 19. VOCAL REGISTERS: CHARACTERISTICS OF VOCAL FOLD ADDUCTION AND VIBRATION Register may include Equivalent terms Vocal folds F0 range Loft register Highest vocal frequancy falsetto Thin,tense lenghtened Minimal vibration 275-1100 Modal register Range of fundamental frequncies used in speaking &singing Chest,head,middle, heavy voice Complete adduction 100-300 Pulse register Lowest range of vocal frequencies laryngeal output is percieved as pulsatile Vocal fry,glottal fry, creaky voice Long closed phase 20-60
- 20. ARTICULATION Tongue Lips Teeth Alveolar ridge (gums behind upper teeth) Soft Palate Hard Palate Velum/uvula The variable action of the tongue on all of the structures listed above results in our ability to articulate different speech sounds A PHONEME is the technical term for a specific sound of speech Phonemes are either vowels or consonants
- 21. VOWELS Vowel sounds There are 5 vowels in the English language (a, e, i, o, u), but there are 12 different vowels sounds (i.e. the letter “i” makes different sounds in the words “miss” and “mice”) The articulation of the different vowel sounds depends on: The point of constriction The degree of constriction The degree of lip-rounding The degree of muscle tension Vowel sounds make up 38% of our speech
- 22. CONSONANTS Consonants of English are classified by: Place of articulation Manner of articulation Degree of Voicing Consonant sounds make up 62% of our speech
- 23. CLASSIFICATION OF CONSONANTS BY PLACE OF ARTICULATION Bilabial: both lips come together (p, b, m, w) Labiodental: lower lip and upper teeth make contact (f, v) Dental: the tongue makes contact with the upper teeth (- th) Alveolar: the tip of the tongue makes contact with the alveolar ridge (t, d, s, z, n, l) Palatal: the tongue approaches the palate (j, r, -sh) Velar: back of the tongue contacts the velum (k, g, -ng) Glottal: this is really an unvoiced vowel (h)
- 24. CLASSIFICATION OF CONSONANTS BY MANNER OF ARTICULATION Manner of articulation refers to the degree of constriction as the consonants begin or end a syllable Stops are defined by complete closure of the lips and subsequent release (p, b) Fricatives use an incomplete closure of the lips to create turbulent noise (f, s, sh) Nasals resonate through the nasal cavity (m, n) Hint: try making these nasal sounds with your nostrils plugged Glides and Liquids are produced when the tongue approaches a point of articulation within the mouth but does not come close enough to obstruct or constrict the flow of air enough to create turbulence (l, r, w)
- 25. VOICED VS. VOICELESS CONSONANTS Voiced consonants are produced with the vocal cords vibrating Voiceless consonants are produced with the vocal cords open Example The sounds /f/ and /v/ are both labiodental fricatives; however, /f/ is voiceless and /v/ is voiced
- 26. RESONANCE Dependent upon the size and shape of the: Vocal Tract Oral Cavity Nasal Cavity The resonant frequency of each of our voices will differ depending on the size and shape of the structures above, much like how the resonance of a cello or bass differs from a guitar, which differs from a ukelele.
- 27. LARYNGEAL DYSTONIA Spasmodic dysphonia (SD) spasmodic dysphonia, a form of movement disorder that involves involuntary "spasms" of the muscles in the vocal folds causing breaks of speech and affecting voice quality. Focal, adult-onset dystonia of laryngeal muscles Intermittent phonatory breaks during speech secondary to spasms Usually task specific - symptomatic when attempting voluntary speech May be asymptomatic during reflexive phonation (coughing, laughing, crying, yawning) Symptoms reduced/absent during singing or whisper
- 28. ASSOCIATIONS May be associated with: Other focal dystonias Blepharospasms, Torticollis, Writer’s Cramp Underlying neurological Parkinson’s, ALS Environmental Infection, trauma, meds Psychogenic stimulus Stress
- 29. DEMOGRAPHICS Affects approximately 1:10,000 Americans Female to male ratio 3:1 up to 8:1 Peak age of onset 35- 45 Positive family history in 12% of affected pt’s
- 30. NEUROPATHOLOGY two different neurologic pathways involved in voice production one being voluntary and the other involuntary. Corticobulbar fibers from the cerebral cortex descend through the internal capsule and synapse on the motor neurons in the nucleus ambiguus.
- 31. alterations in anatomical connectivity of the corticobulbar tract (CBT) descending from the laryngeal/orofacial motor cortex to the brainstem phonatory nuclei. The link between dystonia and basal ganglia dysfunction has been apparent Basal ganglia balance excitation and inhibition of the thalamo-cortical circuit involved in motor execution. This balance is thought to be altered in task-specific dystonias due to reduced GABAergic metabolism and dopaminergic receptor binding leading to excessive motor cortical excitation
- 32. The cerebellum is involved in the motor control via the ventrolateral thalamus and has a modulatory role in coordination of voice and speech production
- 33. NEURAL PATHOLOGY NETWORK . Direct projections from the laryngeal motor cortex (LM1) to the phonatory motor nuclei(nucleus ambiguus, NA) descend via the corticobulbar/corticospinal tract (CBT/CST) The putamen (Put) receives input from the LM1 and projects back to the LM1 via the globus pallidus&vth forming striato- pallido- thalamio cortical loop. . Cerebellar motor input (Cbl) to the LM1 is via the
- 34. Microstructural changes along the CBT/CST as well as in the regions directly or indirectly contributing to the CBT/CST found in this study (dashed areas) may affect voluntary laryngeal control in patients with SD.
- 35. TYPES OF LARYNGEAL DYSTONIAS Adductor – irregular hyperadduction of vocal folds with excessive glottic closure Abductor – incomplete, irregular vocal fold approximation Mixed – both elements are present Adductor laryngeal breathing dystonia (ALBD).
- 36. CLINICAL FEATURES: ADDUCTOR TYPE Most common ~85% of diagnosed cases Choked, strained-strangled voice, with abrupt breaks in phonation in the middle of vowels Breaks are due to hyper-adduction of the folds Difficulty with “We eat eels every day” and “We mow our lawn all year”
- 37. CLINICAL FEATURES: ABDUCTOR TYPE Rare ~15% of patients with SD Breathy, effortful voice with abrupt breaks resulting in whispered elements of their speech. Excessive and prolonged abduction during voiceless consonants (/h/,/s/,/f/,/p/,/t/,/k/) Difficulty with “The puppy bit the tape” and “When he comes home we’ll feed him”
- 38. MIXED TYPE Extremely rare, with symptoms of both adductor and abductor type
- 39. ADDUCTOR LARYNGEAL BREATHING DYSTONIA (ALBD). persistent inspiratory stridor, usually normal voice, and paroxysmal cough. Some patients who have ALBD find it difficult to breathe and swallow at the same time, which results in dysphagia.
- 40. CLINICAL CLASSIFICATION Ludlow and Connor based on constant versus intermittent symptoms and the presence or absence of tremor. ADDUCTOR TYPE (1) constant harsh and tight voice, (2) intermittent pitch and voice breaks in the middle of words, (3) glottal stops with tremor at 4 Hz to 5 Hz in the middle of words
- 41. ABDUCTOR TYPE (1) constant whispering, (2) intermittent breathiness with consonants at the beginnings of words, (3) voice tremor with breathy breaks at 4 Hz to 5 Hz in the middle of words
- 42. Koufman is based on independent visual and acoustic evaluation using fiberoptic laryngoscopy and extensive voice analysis. Focal dystonias (LD) and Nonfocal laryngeal dystonias
- 43. Blitzer and colleagues used a variation of the Koufman and Morrison and Rammage Classification systems. Type 1 hyperadduction is forceful overcontraction at the glottic level only with tight compression of the vocal processes and arytenoids. Type 2 is forceful contraction, including contraction of the false cords. In types 3 and 4, there is supraglottic narrowing in the anteroposterior direction
- 44. Patients with intelligible speech and normal stroboscopic findings are classified as mild. Barely intelligible or unintelligible speech and normal stroboscopy are considered moderate Unintelligible speech who are unable to trigger the strobe are considered severe.
- 45. THANK YOU