Tracheostomy care
•Télécharger en tant que PPTX, PDF•
230 j'aime•210,964 vues

TRACHEOSTOMY care

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Tracheostomy care
Similaire à Tracheostomy care (20)
Plus de THANUJA MATHEW
Plus de THANUJA MATHEW (20)
Dernier
Dernier (20)
Tracheostomy care
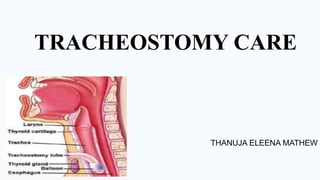
- 1. TRACHEOSTOMY CARE THANUJA ELEENA MATHEW
- 2. INTRODUCTION • A tracheostomy is an opening through the neck into the trachea. A tracheostomy opens the airway and aids breathing. • A tracheostomy may be done in an emergency, at the patient’s bedside or in an operating room. Anaesthesia may be used before the procedure. Depending on the person’s condition, the tracheostomy may be temporary or permanent.
- 3. DEFINITION Tracheostomy care includes changing a tracheostomy inner tube, cleaning tracheostomy site and changing dressing around the site
- 4. INDICATION Obstruction of the mouth or throat Breathing difficulty caused by edema ,injury or pulmonary conditions Airway reconstruction following tracheal or laryngeal surgery Airway protection from secretions or food because of swallowing problems Airway protection after head and neck surgery Long-term need for ventilator support
- 5. PURPOSES 1.To maintain airway patency 2.To prevent infection at the tracheostomy site 3.To facilitate healing and prevent skin excoriation around tracheostomy care. 4.To promote comfort 5.To assess condition of ostomy
- 6. EQUIPMENT I. Tracheostomy care kit containing 1.Gallipots-3 2.Sterile towel 3.Sterile nylon brush/ tube brush 4.Sterile gauze squares 5.Cotton twill ties or tracheostomy tie tapes
- 7. I. A clean tray containing 1.Hydrogen peroxide 2.Normal saline 3.Sterile gloves-1 pairs 4.Face mask and eye shield 5.Waterproof pad
- 9. NURSING ACTION RATIONALE 1. Assess condition of stoma: [ redness, swelling, character of secretions, presence of purulence or bleeding]. Presence of any of these indicates infection and culture examination may be warranted 2.Examine neck for subcutaneous emphysema evidenced by crepitus around the ostomy site. indicates air leak into subcutaneous tissue. 3.Explain procedure to the patient and teach means of communication such as eye blinking or raising a finger to indicate pain or distress. obtain cooperation from patient. 4.Assist patient to a fowlers position and place waterproof pad on chest. promotes lung expansion. Prevents soiling of linen. PROCEDURE
- 10. 5.Wash hands thoroughly. Prevents cross-infection. 6.Assemble equipment’s, a. Open the sterile tracheostomy kit, pour Hydrogen peroxide and sterile normal saline in separate gallipots. a. Open other sterile supplies as needed including sterile applicators, suction kit and tracheostomy care kit a. Put on face mask and eye shield. Hydrogen peroxide and saline removes mucous and crust which promote bacterial growth. Enhances performance phase of procedure. Protects the nurse. 7.Do sterile gloves. Place sterile towel on patient’s chest Maintains aseptic technique.
- 11. 8.Unlock the inner cannula and remove it by gently pulling it out towards you in the line with its curvature. Place the inner cannula in the bowl with hydrogen peroxide suction Hydrogen peroxide moistens and loosens dried secretions. 9.Remove the soiled tracheostomy dressing, discard the dressing and gloves. 10.Clean the flange of the tube using sterile applicators or gauze moistened with hydrogen peroxide and then with normal saline. Use each applicator once only. Using the applicator or gauze once only, avoids contaminating a clean area with a soiled gauze. 11.Clean the stoma tube with the gauze Half strength hydrogen peroxide may be used. Thoroughly rinse the cleaned area using gauze squares moistened with sterile normal saline. Hydrogen peroxide helps to loosen dry crusted secretions. Hydrogen peroxide is irritating to the skin and inhibits healing if not removed thoroughly.
- 12. 12.Dry the stoma tube with dry sterile gauze. An infected wound may be cleaned with gauze saturated with an antiseptic solution, then dried. A thin layer of antibiotic ointment may be applied to the stoma with a cotton swab. May help to clear the wound infection. 13.Cleaning the inner cannula Remove the inner cannula from the soaking solution. Clean the lumen and entire cannula thoroughly using the brush. Rinse the cleaned cannula by rinsing it with sterile normal saline. Thoroughly rinsing is important to remove hydrogen peroxide from inner cannula. Removes solution adhering on the cannula. 14.Replace the inner cannula and secure it in place Insert the inner cannula by grasping the outer Lock the cannula in place by turning the lock into position. This secure the flange of the inner cannula to the outer cannula.
- 13. 15.Apply sterile dressing. Open and refold a 4*4 gauze dressing into a ‘V’ shape and place under the flange on the tracheostomy tube. Do not cut gauze pieces. Ensure that the tracheostomy tube is securely supported while applying dressing. Avoid using cotton- filled 4*4 gauze. Cotton or gauze fibre can be aspirated by the patient potentially creating a tracheal abscess. Excessive movement of the tracheostomy tube irritates the trachea. 16.Change the tracheostomy ties. • Leave the soiled tape in place until the new one is applied Grasp slit end of clean tape and pull it through opening on one side of the tracheostomy tube. Pull the other end of the tape securely thoroughly the slit end of the tracheostomy tube on the other side. Tie the tapes at the side to side of the neck in a square knot. Leaving tape in place ensures that tube will not be expelled if patient coughs or moves. This action provides a secure attachment with knot. Prevents irritation and aids in rotation of pressure site. Excessive tightness compresses jugular veins, decrease blood circulation to the skin and results in discomfort for patient.
- 14. 17.Document all relevant information in the chart Tracheostomy care carried out. Dressing change and • Observations.
- 15. SPECIAL CONSIDERATION 1.Tracheostomy dressing should be done every 8 hours or whenever dressing are soiled 2.Tracheostomy tubes may come with disposable inner cannula or without the inner cannula. If disposable inner cannula is present, then replace the one that is inside with a new one. 3.If only single lumen is present, then suction the tracheostomy tube and clean the neck plate and tracheostomy site.
- 17. NURSES RESPONSIBILITY 1. Tracheostomy dressing should be done every 8 hours or whenever dressing is soiled 2. If disposable inner cannula is present, then replace the one that is inside with a new one. 3. If only single lumen is present, clean the neck plate and tracheostomy site. 4. Emphasize the importance of handwashing before performing tracheostomy care. 5. proper way on how to remove, change, and replace the inner cannula. 6. Check and clean the tracheostomy stoma. 7. Assess for symptoms of infection .
- 18. TEACHER REFERENCE • Jacob Annamma. Rekha. R. clinical nursing procedures the art of nursing practice. 2nd edition. Jaypee publications. New delhi. 2007. Page no: 328-330. • Smeltzer et.al(2011),Brunner and Suddharths Textbook Medical Surgical Nursing, Volume 1 12th Editions, Wolter Kluwer Pvt ,New Delhi pp 778-793 • S M Mogotlane et.al (2009), Jutas Manual of Medical Surgical Nursing, Volume 4, 1st Edition, pp.18-16-18 • Lewis et.al. (2009). Medical Surgical Nursing Assessment And Management Of Clinical Problems.7th edition, Page No.810-71 • Sands’ Phipps Medical Surgical Nursing Health And Illness Perspective, 8th Edition, Page No.903-905
- 19. STUDENT REFERENCE • Smeltzer et.al(2011),Brunner and Suddharths Textbook Medical Surgical Nursing, Volume 1 12th Editions, Wolter Kluwer Pvt ,New Delhi pp 778-793 • Javed Ansari et.al(2015), A Textbook Of Medical Surgical Nursing Pee Vee Publications, Ist Edition, Aurelia Printers, India pp.1433-1437 • S M Mogotlane et.al(2009), Jutas Manual Of Medical Surgical Nursing, Volume 4, 1st Edition, pp.18-16-18 • Lewis et.al.(2009).Medical Surgical Nursing Assessment And Management Of Clinical Problems.7th edition, Page No.810-71 • http://www.nsgmed.com/nursing-procedures • www.upmc.com/patients-visitors/education • https://www.webmd.com