Endoflip after peroral_endoscopic_mytotomy_v0.1
•Télécharger en tant que DOCX, PDF•
1 j'aime•791 vues


Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Endoflip after peroral_endoscopic_mytotomy_v0.1
Similaire à Endoflip after peroral_endoscopic_mytotomy_v0.1 (20)
Dernier
Dernier (20)
Endoflip after peroral_endoscopic_mytotomy_v0.1
- 1. Use of EndoFLIP system for the evaluation of the effects of Peroral Endosqcopic Myotomy. Results of a prospective observational study on a consecutive series of patients BACKGROUND AND AIMS Achalasia is an rare esophageal disease characterized by absence of efficacious peristalsis of the esophageal body and impaired relaxation of the lower esophageal sphincter (LES) in response to swallowing. ( Ghoshal UC, Daschakraborty SB, Singh R. Pathogenesis of achalasia cardia. World J Gastroenterol. 2012 Jun 28;18(24):3050-7) Achalasia is characterized by the progressive degeneration of the neurons of the myoenteric Auerbac’s plexus. ( Chuah SK, Hsu PI, Wu KL, Wu DC, Tai WC, Changchien CS. 2011 update on esophageal achalasia. World J Gastroenterol. 2012 Apr 14;18(14):1573-8.) Degeneration is irreversible, and all the available treatments - medical, endoscopic and surgical – aim to relief the symptoms of achalasia (dysphagia, regurgitation, chest pain and weight loss) by reducing the basal and swallow induced residual LES pressure. (Katada N, Sakuramoto S, Yamashita K, Shibata T, Moriya H, Kikuchi S, Watanabe M. Recent trends in the management of achalasia. Ann Thorac Cardiovasc Surg. 2012;18(5):420-8.) The classic surgical treatment of achalasia is Heller myotomy associated with and an antireflux wrap. (Allaix ME, Patti MG. What is the Best Primary Therapy for Achalasia: Medical or Surgical Treatment? Who Owns Achalasia? J Gastrointest Surg. 2013 Jun 19)
- 2. The disruption of the muscular fibers of the LES by using endoscopic pneumatic dilation with large caliber balloons offers excellent short term results, with a minimal complication- rate and invasiveness. (Yaghoobi M, Mayrand S, Martel M, Roshan-Afshar I, Bijarchi R, Barkun A. Laparoscopic Heller's myotomy versus pneumatic dilation in the treatment of idiopathic achalasia: a meta-analysis of randomized, controlled trials. Gastrointest Endosc. 2013 May 14) However, the benefits of balloon dilations seem to vanish with time, and in young patients. (Boeckxstaens GE, Annese V, des Varannes SB, Chaussade S, Costantini M, Cuttitta A, Elizalde JI, Fumagalli U, Gaudric M, Rohof WO, Smout AJ, Tack J, Zwinderman AH, Zaninotto G, Busch OR; European Achalasia Trial Investigators Pneumatic dilation versus laparoscopic Heller's myotomy for idiopathic achalasia. N Engl J Med. 2011 May 12;364(19):1807-16. doi: 10.1056/NEJMoa1010502.) More recently Peroral Endoscopic Myotomy has been introduced in the clinical practice as as an endoscopic alternative to surgical myotomy.( Inoue H, Minami H, Kobayashi Y, et al. Peroral endoscopic myotomy(POEM) for esophageal achalasia. Endoscopy 2010;42:265- 71). POEM may offer the same long term benefits of surgical myotomy, with the minimal invasiveness of an endoscopic transoral procedure. POEM is gaining international consensus, even if few data are available for a long term evaluation. (Stavropoulos SN, Modayil RJ, Friedel D, Savides T. The International Per Oral Endoscopic Myotomy Survey (IPOEMS): a snapshot of the global POEM experience. Surg Endosc. 2013 Apr 3) The efficacy of the therapeutic interventions for achalasia is usually measured by symptoms evaluation, appearance of Esophago-Gastric Junction (EGJ) at EsophagoGastroDuodenoscopy (EGD) and timed esophagograms, and by esophageal manometry. The EndoFLIP (Endolumenal Functional Lumen Imaging Probe) System is a new technology that provides real-time measurements of the diameter of EGJ and of its cross sectional area (Regan J, Walshe M, Rommel N, Tack J, McMahon BP.New measures of upper esophageal sphincter distensibility and opening patterns during swallowing in healthy subjects using EndoFLIP®. Neurogastroenterol Motil. 2013 Jan;25(1):e25-34) (Alqudah MM, Gregersen H, Drewes AM, McMahon BP. Evaluation of anal sphincter resistance and distensibility in healthy controls using EndoFLIP ©. Neurogastroenterol Motil. 2012 Dec;24(12):e591-9)
- 3. through a specific catheter with balloon attached at the distal end, using specific algorithms and impedence planimetry. EndoFLIP may allow to immediately evaluate the effects of any therapeutic interventions on the LES and EGJ, including antireflux procedure (Video. Perretta S, Dallemagne B, McMahon B, D'Agostino J, Marescaux J Improving functional esophageal surgery with a "smart" bougie: Endoflip. Surg Endosc. 2011 Sep;25(9):3109) (Lin Z, Kahrilas PJ, Xiao Y, Nicodème F, Gonsalves N, Hirano I, Pandolfino JE. Functional luminal imaging probe topography: an improved method for characterizing esophageal distensibility in eosinophilic esophagitis. Therap Adv Gastroenterol. 2013 Mar;6(2):97-107) , and treatment of achalasia (Massey BT. EndoFLIP assessment of achalasia therapy: interpreting the distensibility data is a bit of a stretch. Gastroenterology. 2013 Apr;144(4):e17-8.) . However few studies evaluate the possible benefits of the use of EndoFLIP after POEM . (Verlaan T, Rohof WO, Bredenoord AJ, Eberl S, Rösch T, Fockens P. Effect of peroral endoscopic myotomy on esophagogastric junction physiology in patients with achalasia. Gastrointest Endosc. 2013 Jul;78(1):39-44) (Rieder E, Swanström LL, Perretta S, Lenglinger J, Riegler M, Dunst CM. Intraoperative assessment of esophagogastric junction distensibility during per oral endoscopic myotomy (POEM) for esophageal motility disorders. Surg Endosc. 2013 Feb;27(2):400-5) Aims of this prospective observational study is to report on the effects of POEM on the LES, as evaluated with EndoFLIP. METHODS All the patients who underwent POEM in a single tertiary referral center between April 2013 and July 2013 were enrolled in the study, POEM was offered to patients with a confirmed diagnosis of achalasia and an Eckardt score greater than 3. Diagnostic workup for achalasia, included, as usual, high resolution manometry, timed barium esophagograms, and EGD. POEM technique POEM was performed by two endoscopist (GC and PF) according the technique previously described by Inoue et al. (Endoscopy 2010). The mucosa of the esophagus was lifted with a 10% glycerol solution, and incised approximately 10-13 cm above the GEJ. A
- 4. TT-knife was used to create a tunnel into the esophageal submucosal, extended for three cm beyond the GEJ. After dissection was completed, myotomy was performed, and included preferably the circular bundles of the esophageal and cardial muscularis propria. The mucosal defect was sutured with endoscopic clips. EndoFLIP system and catheter The EndoFLIP® System technology uses impedance planimetry to characterize the geometry of cross sectional measurement areas. Impedance planimetry uses AC voltage measurements made between pairs of electrodes to estimate the extent of the diameter of the medium (a conductive fluid) at the mid-point between those electrodes. This can be done provided the voltage drop across the medium is generated from a constant AC current source and the conductivity of the medium is constant and known for a given temperature. If the conductive medium is contained in a flexible balloon and an array of voltage electrodes used, the shape of the balloon can be reproduced based on the voltage readings. This is the basis of the EndoFLIP imaging technique. (Picture 1) The EndoFLIP EF-825 catheter was used for the study. This catheter has attached at the distal end a 14cm long balloon, with 17 electrodes (5 mm apart) inside providing an 8 cm long image field, for volume controlled measurements. No pressure sensors are embedded in this catheter. EndoFLIP measurements were performed on the same day, immediately before and immediately after the POEM procedure, with the patient under general anesthesia and oro- tracheal intubation. The catheter was advanced transorally to the stomach, alongside the endoscope, under direct visual control. The balloon was inflated with 30mL of balanced saline solution, and pulled back into the EGJ to a point where the EGJ was observed to be located centrally within the balloon. The narrowest cross-sectional area identified the lower esophageal sphincter and the GEJ, and was used as reference diameter. Still images of the EndoFLIP measurements were acquired and stored for comparisons, before and after the POEM. Management after POEM and follow-up Patients resumed oral feeding 1 or 2 days after POEM and were discharged on the 3rd or 4th post-operative days. Follow-up visits for symptoms assessment were performed 30 days after the procedure. At 3-month follow-up patients underwent again symptoms evaluation, esophageal high resolution manometry and pH-metry.
- 5. Data analysis and statistics Demographics, preoperative and procedural data, results of the EndoFLIP measurements and follow-up data were recorded into a prospectively collected database on Microsoft Excel, encrypted and stored. The data collected before and after POEM were compared with the preoperative and post- operative EndoFLIP measurements. Data are presented as mean + standard deviation when parametric and as median (interquartile range [IQR]) when nonparametric. Parametric variable were tested by using a t test. Paired nonparametric data were tested by using the Wilcoxon signed rank test. A P value of .05 was considered as statistically significant. RESULTS During the study periods 23consecutive patients (12 males, mean age 51.7 years) underwent POEM and EndoFLIP, and were enrolled in the study. Mean Eckardt score before POEM was 8.6. 13 patients had a type I achalasia at HRM; 10 a type-II. Preoperative mean basal LES pressure was XX mmHg and mean 4sIRP was XXXmmHg. The procedure were completed successfully in 21 of 23 patients. In one patients, with history of mammalian cancer and mediastinal irradiation mucosal lifting failed and POEM procedure aborted; the patient underwent pneumatic dilation using a 30mm balloon. EndoFLIP was successfully performed in all the cases. The day after the procedure the patients underwent EGD and esophageal Gastrografin® study, demonstrating no complications, and the patients were fed with a soft diet. Patients were discharged an average 3 days after the procedure. EndoFLIP measurements Baseline EndoFLIP data are available for all the patients. Before POEM, the EGJ diameter and cross sectional area - as measured with EndoFLIP and a balloon inflated with 30ml of saline solution – were on average 5.1 mm (+ 1.8 SD) and 32.9 mm2 (+ 23.7SD), respectively. After treatment, the mean diameter and cross-sectional area of the EGJ were substantially increased, 11.3 mm (+ 0.35SD) and 102.38 mm2 (+ 28.9 SD) respectively. All the patients had a variation of more of XX mm in diameter before and after POEM.
- 6. In a patient, after the initial myotomy, the diameter of the EGJ was not substantially wider compared to the preoperative results (6.7 mm vs 7.1 mm, respectively). The endoscope was thus reinserted in the submucosal tunnel, and some more circular bundles of the LES were cut using electrocoagulation. At the final measurement using EndoFLIP, the mean diameter of LES at 30ml was now 12.7 mm. Follow-up Only a short follow.-up is available for the patients. No complications occurred in the study population. After a mean of XX months (xx weeks – xx months), the entire study population referred complete dysphagia relief, with a mean Eckard score of XX. Non symptoms of GERD were referred by the patients. pH-metry reveal pathological reflux total reflux time > 4%) in xx% of patients. At the 3-month HRM, average basal LES pressure was xx mmHg (+ SD) and 4sIRP xx mmHg (+ SD). At univariate analysis, no statistically significant correlations were observed between the postoperative EndoFLIP measurement of the EGJ, and the Eckardt score, GERD incidence and LES pressures. DISCUSSION POEM is now considered effective and safe for the treatment of esophageal achalasia. The aim of any therapy of achalasia, surgical or endoscopic, is to improve the esophageal emptying, by reducing the basal- and swallow-induced resting LES pressure, by improving the compliance of the EGJ to the passage of food. Previous studies demonstrated that the long term benefits of surgical and endoscopic treatment of achalasia are directly related with the reduction of the basal LES pressure. Recurrences of dysphagia have been observed more frequently in case of LES pressure > 10mmHg. Some authors support re-interventions after pneumatic dilation in case the LES pressure after treatment is > 10mmHg, even in case of absence of symptoms, to prevent recurrences. Unfortunately manometric studies cannot be performed during POEM, being the patients under general anesthesia, and any evaluation of the effects of myotomy on LES pressure and esophageal emptying should be performed in the post-operative time.
- 7. Some authors demonstrated that the distensibility of the EGJ can substantially affects the esophageal emptying, and this parameter could correlate with long term efficacy and adverse events (including GERD). EndoFLIP allows a real-time measurement of the diameter of the esophagus and of the EGJ by using an impedentiometry-based catheter, with a distal balloon that is inflated with a certain volume of saline solution. The probe used for the measurements is thin, has a very soft, atraumatic and flexible tip, and can be easily pushed through the cardia before and after POEM. Because of the small caliber, the position of the catheter can be check using an endoscope alongside the probe. The measurement of the diameters and cross- sectional areas using the balloon based catheter does not require any collaboration by the patient (swallowing, breathing…), and thus EndoFLIP can be used during the operation under general anesthesia, to tailor the myotomy and verify the effects of POEM on the GEJ and LES. Currently during POEM, the effects and completeness of myotomy can be only assessed subjectively and empirically, by evaluating the appearance of myotomy at EGD and by passing the endoscope through the cardia, trying to appreciate any resistance to the transit. In order to have a complete myotomy at the level of the LES, submucosal dissection and myotomy are usually extended for 2-3 cm beyond the cardias on the gastric wall. However, again endoscopic measurements are subjective and imprecise, and be affected by many bias. On the counterpart, the possibility to measure the diameter of the GEJ and distensibility before and after the POEM can be particularly useful to reveal cases of incomplete myotomy, before the closure of the entry of submucosal tunnel with clips. In one of our cases, even if the myotomy seemed complete at the end of the procedure, EndoFLIP did not reveal any substantial change of the diameter of the GEJ, with the balloon inflated at 30ml. Hence, some additional muscular bundles were cut at the level of the GEJ, with a substantial improvement of diameter at the end. Differently from the other ones, the EndoFLIP probes used in this study (EF-825) does not measure pressure, and consequently a real distensibilty of the EGJ has not been assessed during the study. Even if attractive from a scientific point of view, “distensibility” (by meaning of a direct function of pressure – mm2/mmHg), can be practically meaningless, since surgeon and endoscopists want to set the lumen size and not
- 8. compliance of EGJ. Thus, the “diameter of GEJ” or its “crossectional area” are more intuitive parameters, and probably more useful during the procedure. Measuring the diameter that the EGJ opens out to with 30mL in the balloon is giving us a different measure of distensibility, how much the EGJ opens for a given volume in the balloon. 30mL simulates a bolus pressure of around 10-15mmHg, probably more similar to what happens during physiological swallowing. Furthermore, pressure is very variable and susceptible to changes for the smallest of reasons. Therefore the diameter or the cross- sectional area are more robust measurements One of the most common adverse events after POEM is GERD. Differently from surgical Heller Myotomy, an antireflux procedure is not performed after POEM, leading to a possible increased incidence of GERD. Incidence of GERD is very variable in published series, from 5% to 46%. A wider opening of the GEJ, as seen with the EndoFLIP system, may theoretically favor GERD, as demonstrated by previous studies. The average diameter of the GEJ after POEM varied in the literature from xx to xx. In the present study the GEJ diameter passed from xx mm preoperatively to xx postoperatively, similarly to previous studies. However, it is still unknown which should be the correct EGJ diameter that allow a quick esophageal emptying by avoiding at the same time GERD. Furthermore, the effects of POEM on the distensibility of the EGJ are often unpredictable, and not really controllable, and unfortunately it is not possible to narrow and restrict the GEJ after POEM. EndoFLIP system is a safe and effective technology for the evaluation of the effects of myotomy on the GEJ and LES. The data obtained from the measurements of the diameter of the lower esophageal sphincter associated with clinical and instrumental data of the follow-up of patients may be useful to improve POEM technique by assessing and establishing the correct diameter of the EGJ that allow a quick esophageal emptying with a minimal the risk of GERD. AGGIUNGERE UN PARAGRAFO SU STUDI PRECEDENTI SU ENDOFLIP E POEM
- 10. I know we have done some cases with you where the minimum diameter started out above 8mm, and for these cases I personally believe that the POEM benefit is derived not from removing outflow obstruction, but something else in the procedure. As a rule of thumb, in fundoplication, a target of around 8mm at crural repair and 6-6.5mm after the wrap seems to be about right. One would expect the GEJ to be set looser in an achalasic with poor peristalsis, so 8mm seems to make sense in a qualitative sense. In terms of extremes, most Heller pts seem to come in around 5mm pre-procedure, whereas bad GERD patients come in around 10mm (think of a 9.2mm scope passing easily through the junction). So measurement of diameter is a more practical intra-operative and cost effective tool. We do have another catheter that also measures balloon pressure and distensibility (EF-325). Pressure is vary variable and susceptible to changes for the smallest of reasons. Say you had a cross sectional area of 50mm2 and the pressure varied by 3mm (very little) e.g. from 10 to 13, the distensibility would go form 50/10 (= 5) to 50/13 (=3.85) .. a change of 30%. I therefore also feel that diameter is a more robust measurement. Most people doing work with pressure on EndOFLIP will tell you that this takes a lot of post-processing and filtering of the data. Personally I am little less than convinced in relation to its robustness. You are correct. The EF-825 does not measure pressure. Whereas some people are measuring distensibility, most of our day to day work (and most recent fundoplication work) is focussed on the cross sectional area or diameter of the junction (please see the attached presentation as it relates to fundoplication). The reason for this is that setting the compliance of the junction is a bit meaningless, since surgeons/endoscopists want to set the lumen size. e.g. if I told you the lumen size was 5mm but the distensibility was 2.8, what would you do, well you likely would open the lumen out to 9+mm of course. So whereas distensibility is nice science, it is not really assisting in a real practical sense during the procedure (though maybe perhaps it is a nice check at the end). We are trying to encourage the use of diameter as it is more intuitive and practical i.e. you want to open or close the junction to establish a new geometry as
- 11. opposed to creating a new degree of spring-iness (thought he latter might be nice to know, the former will be the real procedural intent !). EndoFLIP in POEM - Diametro PRE…..Diametro POST (Tab 1) - CSA PRE…………..CSA POST (Tab 2) - Caso particolare di Coppola Giuseppa che diametro PRE simile a diametroPOST rientrati ed estesa miotomia a tutto spessore con Diametro POST POST allargato. EndoFLIP in Pneumatic Dilation - Diametro PRE…..Diametro POST (Tab 3) - CSA PRE…………..CSA POST (Tab 4)
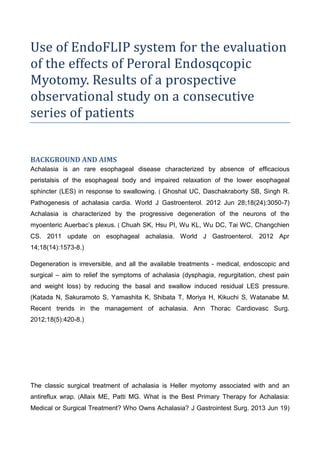
- 13. Picture 3 Se riesci a fare 3 frame consecutivi da filmato di posizionamento e gonfiaggio EndoFlip. Tab 1 POEM : Diametri singoli PRE e POST , Diametro medio PRE e POST 0 2 4 6 8 10 12 14 16 Diametro PRE Diametro POST 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
- 14. Tab 2 POEM : CSA singoli PRE e POST CSA medio PRE e POST 0 2 4 6 8 10 12 Med Diametro PRE Med Diametro POST Diam 0 20 40 60 80 100 120 140 160 180 CSA PRE CSA POST 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
- 15. Tab 3 Pneumatic Dilation : Diametri singoli PRE e POST , Diametro medio PRE e POST 0 20 40 60 80 100 120 Med CSA PRE Med CSA POST CSA
- 16. Tab 4 Pneumatic Dilation : CSA singoli PRE e POST , CSA medio PRE e POST 0 20 40 60 80 100 120 140 160 180 200 Diametro PRE Diametro POST 1 2 3 0 20 40 60 80 100 120 Med CSA PRE Med CSA POST CSA