Progressive macular hypomelanosis PMH
•Télécharger en tant que PPTX, PDF•
3 j'aime•4,321 vues

Progressive macular hypomelanosis (PMH) is a common skin disorder that is often misdiagnosed.

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Progressive macular hypomelanosis PMH
Similaire à Progressive macular hypomelanosis PMH (20)
Plus de Yapa
Plus de Yapa (20)
Dernier
Dernier (20)
Progressive macular hypomelanosis PMH
- 1. PMH by Yapa Wijeratne Faculty of Medicine University of Peradeniya Sri Lanka
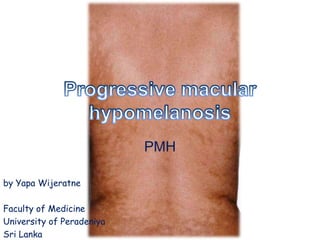
- 2. • Progressive macular hypomelanosis (PMH) is a common skin disorder that is often misdiagnosed. • characterized by ill defined, nummular, symmetrically localized, hypopigmented macules on sebum-rich areas of the skin. • Various authors have written about similar skin disorders, referring to them by different names, but we believe that all these similar disorders are part of the same entity.
- 4. PMH is characterized by 1. Ill-defined nummular, 2. Non-scaly hypopigmented spots on the trunk, 3. Often confluent in and around the midline, 4. Rarely extending to the proximal extremities and neck/head region. 5. There is no itch, pain, or preceding inflammation.
- 5. • PMH has a worldwide distribution; however, it is more often identified in Black people living in or originating from tropical countries. • It is also more often seen in young females. • The natural history of PMH is stable disease or perhaps slow progression over decades, with spontaneous disappearance after mid- life.
- 6. • Extensive pityriasis alba is probably identical with PMH and we suggest discontinuation of use of the former term on the grounds that extensive pityriasis alba is histologically and clinically different from classical pityriasis alba, which is basically an eczematous type of disorder.
- 7. • PMH is characterized histologically by diminished pigment in the epidermis and a normal-looking dermis. • Electron microscopy shows a shift from large melanosomes in normal-looking skin to small aggregated, membrane-bound melanosomes in hypopigmented skin. • PMH should be differentiated from other disorders with hypopigmentation on the trunk such as pityriasis versicolor.
- 8. • We propose that Propionibacterium acnes bacteria living in hair follicles are the cause of PMH as a result of production of a hypothetical depigmenting factor. • This hypothesis is based on: • (i) the presence of a red follicular fluorescence in the hypopigmented spots and the absence of this phenomenon in normal skin when examined under a Wood's light in a dark room;
- 9. • (ii) cultivation of P. acnes from the follicles in the hypopigmented spots but not from follicles in normal-looking skin; and • (iii) improvement of the disorder after elimination of these micro-organisms with topical antimicrobial treatment in combination with UVA light.
- 10. • Currently, the treatment of choice of PMH is application of 1. 1% clindamycin lotion during the daytime, 2. 5% benzoyl peroxide gel at night-time, and 3. UVA light irradiation 3/week for a period of 12 weeks. • There is insufficient information available as yet to comment on the recurrence rate after therapy.