![DISCUSSION: In third world countries, ameloblastoma
distinguishes by its volume on patients with a poor buccodental
hygiene [1,2].
Literature reports that:
- most common neoplasm arising from the primary odontogenic, or
tooth forming tissue; expand within the jaw and displace bone,
teeth, and roots
- slow growing non-encapsulated tumours, usually asymptomatic
until large size is achieved [3]
- high frequency in African countries [1,2] Fig 4: per-operative aspect
- 3 histological patterns: follicular, plexiform and mixed [4, 5]
- 3 radiological patterns: polycystic, monocystic and solid [5]
- mandibular localization: 85% of cases [5]
- some patterns more reccurent: polycystic and follicular: our case Fig 5: giant ameloblastoma
measuring 20 x 12 x 13 cm
→ Diagnosis relatively clear in patients with jaw masses of this extreme
size and with characteristic findings on imaging studies.
→ Differential diagnosis: fibrous dysplasia or histiocytosis
→ Therapy for giant ameloblastoma =>surgical resection [5]
→ Enucleation inadequate for large lesions ( high rate of recurrence ):
bony surgical margins of 1 to 2 cm recommended [6]
→ Caution should be exercised, however, because
histologic transformation can occur (both metastatic and
malignant transformation potential) [7,8]
CONCLUSION: This case report illustrates the importance
of adequate radical resection to avoid recurrence. Therefore,
it is important to emphasize the need for long term
periodic follow-up which is very difficult in under- Fig 6a, 6b & 6c: postoperative aspect: without reconstruction
medicalized countries. Ameloblastoma implicates also ABSTRACT
diagnosis and therapeutic challenges in these countries.
REFERENCES The authors report a historical case of a recurrent giant
[1] GADEGBEKU AS, CREZOIT GBE, ADOU A, ANGOH Y, MAREGA FB.
L’améloblastome en milieu africain. Rev Stomatol Chir Maxillofac 1994;95:70-73. ameloblastoma of the mandible. Six years ago a recurrence
[2] CHIDZONGA MM, LOPEZ PEREZ VM, PORTILLA ALVAREZ AL. Ameloblastoma: the appeared after partial surgery, this ameloblastoma developed
Zimbabwean experience over 10 years. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
1996;82:38-41. from the left half-mandible blowing out the mandible and the
[3] DUPUIS A, DINER PA, MICHAUD J. Améloblastome géant. A propos d’un cas de Maxillary bone. The pathological study revealed a follicular
localisation mandibulaire. Rev Stomatol Chir Maxillofac. 1983;84:218-21.
[4] OLAITAN AA, AROLE G, ADEKEYE EO. Recurrent ameloblastoma of the jaws. A ameloblastoma without character of malignity. This
follow-up study. Int J Oral Maxillofac Surg. 1998;27:456-60. unusual case points out to us the therapeutic difficulties at the
[5] KIM SG, JANG HSJ. Ameloblastoma: a clinical, radiographic, and histopathologic analysis
of 71 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91:649-53. time of the recurrences of ameloblastomas on the one hand
[6] NAKAMURA N, HIGUCHI Y, MITSUYASU T, SANDRA F, OHISHI M. Comparison of and the difficulties of follow-up of patients in tropical area
long-term results between different approaches to ameloblastoma. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 2002;93:13-20. on the other hand.
[7] ROBINSON HBG. Ameloblastoma: a survey of three hundred and seventy-nine cases from
the literature. Arch Pathol 1937;23:831-43.
[8] SLOOTWEG PJ, MULLER H. Malignant ameloblastoma or ameloblastic carcinoma. Oral Key words: ameloblastoma, mandible, recurrence, giant
Surg 1984;57:168-76. tumor, surgery.](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Giant Ameloblastoma
Similaire à Giant Ameloblastoma (20)
Plus de aliabbas07
Giant Ameloblastoma
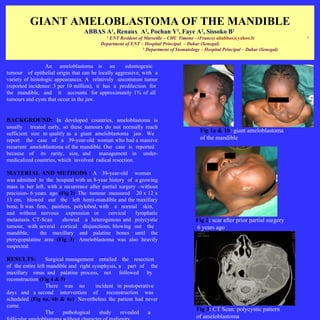
- 1. GIANT AMELOBLASTOMA OF THE MANDIBLE ABBAS A , Renaux A , Pochan Y , Faye A , Sissoko B 1 2 3 2 2 1 ENT Resident of Marseille – CHU Timone - (France) aliabbas@yahoo.fr 2 Department of ENT – Hospital Principal – Dakar (Senegal) 3 Department of Stomatology – Hospital Principal – Dakar (Senegal) An ameloblastoma is an odontogenic tumour of epithelial origin that can be locally aggressive, with a variety of histologic appearances. A relatively uncommon tumor (reported incidence: 3 per 10 million), it has a predilection for the mandible, and it accounts for approximately 1% of all tumours and cysts that occur in the jaw. BACKGROUND: In developed countries, ameloblastoma is usually treated early, so these tumours do not normally reach sufficient size to qualify as a giant ameloblastoma jaw. We Fig 1a & 1b: giant ameloblastoma report the case of a 39-year-old woman who had a massive of the mandible recurrent ameloblastoma of the mandible. Our case is reported because of its rarity, size, and management in under- medicalized countries, which involved radical resection. MATERIAL AND METHODS : A 39-year-old woman was admitted to the hospital with an 8-year history of a growing mass in her left, with a recurrence after partial surgery –without precision- 6 years ago (Fig 2). The tumour measured 20 x 12 x 13 cm, blowed out the left hemi-mandible and the maxillary bone. It was firm, painless, polylobed, with a normal skin, and without nervous expression or cervical lymphatic metastasis. CT-Scan showed a heterogenous and polycystic Fig 2: scar after prior partial surgery tumour, with several cortical disjunctions, blowing out the 6 years ago mandible, the maxillary and palatine bones until the pterygopalatine area (Fig 3). Ameloblastoma was also heavily suspected. RESULTS: Surgical management entailed the resection of the entire left mandible and right symphysis, a part of the maxillary sinus and palatine process, not followed by reconstruction (Fig 4 & 5). There was no incident in postoperative days and a second intervention of reconstruction was scheduled (Fig 6a, 6b & 6c). Nevertheless the patient had never come. Fig 3: CT Scan: polycystic pattern The pathological study revealed a of ameloblastoma
- 2. DISCUSSION: In third world countries, ameloblastoma distinguishes by its volume on patients with a poor buccodental hygiene [1,2]. Literature reports that: - most common neoplasm arising from the primary odontogenic, or tooth forming tissue; expand within the jaw and displace bone, teeth, and roots - slow growing non-encapsulated tumours, usually asymptomatic until large size is achieved [3] - high frequency in African countries [1,2] Fig 4: per-operative aspect - 3 histological patterns: follicular, plexiform and mixed [4, 5] - 3 radiological patterns: polycystic, monocystic and solid [5] - mandibular localization: 85% of cases [5] - some patterns more reccurent: polycystic and follicular: our case Fig 5: giant ameloblastoma measuring 20 x 12 x 13 cm → Diagnosis relatively clear in patients with jaw masses of this extreme size and with characteristic findings on imaging studies. → Differential diagnosis: fibrous dysplasia or histiocytosis → Therapy for giant ameloblastoma =>surgical resection [5] → Enucleation inadequate for large lesions ( high rate of recurrence ): bony surgical margins of 1 to 2 cm recommended [6] → Caution should be exercised, however, because histologic transformation can occur (both metastatic and malignant transformation potential) [7,8] CONCLUSION: This case report illustrates the importance of adequate radical resection to avoid recurrence. Therefore, it is important to emphasize the need for long term periodic follow-up which is very difficult in under- Fig 6a, 6b & 6c: postoperative aspect: without reconstruction medicalized countries. Ameloblastoma implicates also ABSTRACT diagnosis and therapeutic challenges in these countries. REFERENCES The authors report a historical case of a recurrent giant [1] GADEGBEKU AS, CREZOIT GBE, ADOU A, ANGOH Y, MAREGA FB. L’améloblastome en milieu africain. Rev Stomatol Chir Maxillofac 1994;95:70-73. ameloblastoma of the mandible. Six years ago a recurrence [2] CHIDZONGA MM, LOPEZ PEREZ VM, PORTILLA ALVAREZ AL. Ameloblastoma: the appeared after partial surgery, this ameloblastoma developed Zimbabwean experience over 10 years. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:38-41. from the left half-mandible blowing out the mandible and the [3] DUPUIS A, DINER PA, MICHAUD J. Améloblastome géant. A propos d’un cas de Maxillary bone. The pathological study revealed a follicular localisation mandibulaire. Rev Stomatol Chir Maxillofac. 1983;84:218-21. [4] OLAITAN AA, AROLE G, ADEKEYE EO. Recurrent ameloblastoma of the jaws. A ameloblastoma without character of malignity. This follow-up study. Int J Oral Maxillofac Surg. 1998;27:456-60. unusual case points out to us the therapeutic difficulties at the [5] KIM SG, JANG HSJ. Ameloblastoma: a clinical, radiographic, and histopathologic analysis of 71 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91:649-53. time of the recurrences of ameloblastomas on the one hand [6] NAKAMURA N, HIGUCHI Y, MITSUYASU T, SANDRA F, OHISHI M. Comparison of and the difficulties of follow-up of patients in tropical area long-term results between different approaches to ameloblastoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;93:13-20. on the other hand. [7] ROBINSON HBG. Ameloblastoma: a survey of three hundred and seventy-nine cases from the literature. Arch Pathol 1937;23:831-43. [8] SLOOTWEG PJ, MULLER H. Malignant ameloblastoma or ameloblastic carcinoma. Oral Key words: ameloblastoma, mandible, recurrence, giant Surg 1984;57:168-76. tumor, surgery.