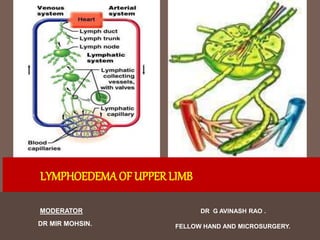
5. Histology
No basement membrane
Wide spaced endothelial cells
Connective tissue content increases as depth increases
Communication between deep and superficial system
are few
Don’t function in normal people
Flow can be deep to superficial
6. DEF-
The cell wall of lymphatic collecting channels contain valves to
prevent backflow of the lymphatic fluid. The sections between
these valves, called LYMPHANGIONS.
Tissue fluid drainage occurs in distinct regions of the body
called LYMPHOTOMES.
7. Factors for lymphatic flow
Interstitial pressure gradient
Lymphangions contraction
Valves
Muscular contraction
Compression by adjacent pulsation
Negative pressure by intrathoracic and intraabdominal respiratiory
excursion
Rapid flow in veins
8. Course of drainage
Dermis (valveless channels-
Prelymphatics)
Subdermal (valved lymphatics)
Large valved Epifascial Channels
Subfascial lymphatics
9. If obstruction in epifascial
system
Backflow to subdermal plexus
Cross over to the next quadrant
Subdermal edema: peau de orange
10. Paired axillary system
No lymphatic circulation across the watersheds
where the direction of lymphatic flow changes
Minimal communication in midline
11. LYMPH VESSELS
The lymph vessels draining the lymph from the upper limb in the
body are split Into 2 groups:
1. Superficial
2. Deep
12. SUPERFICIAL LYMPH VESSELS
The superficial lymph vessels are in the subcutaneous tissue,
accompany the superficial veins.
They course upwards in the direction of the axilla. Most of them
end in the axillary lymph nodes.
Those from lateral side of the limb and lateral 2 digits follow the
cephalic vein and drain into theinfraclavicular lymph nodes.
13. Those from medial side of the limb and medial 3 digits follow the
basilic vein and drain into the lateral group of axillary nodes.
A number of the medial lymph vessels terminate in the
supratrochlear or epitrochlear nodes, that are situated just above
the medial epicondyle along the basilic vein.
A couple of lymph vessels drain the thumb end in the
deltopectoral lymph nodes.
The efferents from these nodes pierce the clavipectoral fascia to
drain in the apical group of axillary nodes
14. Just about all the superficial lymph vessels of the upper
limb drain into lateral group of axillary nodes.
Lymph from palm is drained into the lymph plexus on the
dorsum of the hand.
15. Axillary LN dissection should spare infraclavicular
Pathway
Post ALND important to immobilize operated site
with compression ASD for formation of new
lympholymphatic anastomoses
16. DEEP LYMPH VESSELS
The deep lymph vessels are much less numerous in relation
to the superficial lymph vessels.
They drain structures being located deep to deep fascia,
i.e. muscles.
The deep lymph vessels course along the arteries and
drain into the lateral group of the axillary lymph nodes.
17. LYMPH NODES
• The lymph nodes draining the upper limb are split into 2
groups:
–(a) Superficial and
–(b) Deep.
18. SUPERFICIAL LYMPH NODES
• They are located in the superficial fascia, along with the superficial vein. All these are
as follows:
1. Infraclavicular nodes, 1 or 2 in number, are located on
the clavipectoral fascia along the cephalic vein. They drain lymph from thumb and
upper part of the breast.
2. Deltopectoral nodes, are located in the deltopectoral groove along the
cephalic vein just before it pierces the deep fascia.
– It drains the lymph from the breast and adjoining small structures.
– It’s thought to be displaced infraclavicular node.
3. Superficial cubital / supratrochlear nodes are located 5 cm above the
medial epicondyle along the basilic vein. They drain the lymph from the ulnar side of
the hand and forearm.
19.
20. DEEP LYMPH NODES
• The deep lymph nodes are as follows:
• Axillary lymph nodes are existing in the axilla and are split into
5 sets. These are main lymph nodes of the upper limb.
• A few other deep lymph nodes are located on the following sites:
– Along the medial side of the brachial artery.
– In the cubital fossa, in the bifurcation of the brachial artery (named deep
cubital node).
– Occasionally along the arteries of the forearm.
21. LYMPH NODES
• The majority of the upper lymph nodes are located in the
axilla. They can be divided anatomically into 5 groups:
1. Pectoral (anterior)
2. Subscapular (posterior)
3. Humeral (lateral)
4. Central
5. Apical
22.
23.
24. Axillary lymph nodes
1. Pectoral (anterior) – 3-5 nodes, located in the medial wall of the axilla.
They receive lymph primarily from the anterior thoracic wall, including
most of the breast.
2. Subscapular (posterior) – 6-7 nodes, located along the posterior axillary
fold and subscapular blood vessels. They receive lymph from the posterior
thoracic wall and scapular region.
3. Humeral (lateral) – 4-6 nodes, located in the lateral wall of the axilla,
posterior to the axillary vein. They receive the majority of lymph drained
from the upper limb.
25. 4. Central – 3-4 large nodes, located near the base of the axilla (deep to
pectoralis minor, close to the 2nd part of the axillary artery). They receive
lymph via efferent vessels from the pectoral, subscapular and humeral
axillary lymph node groups.
5. Apical – Located in the apex of the axilla, close to the axillary vein and
1st part of the axillary artery. They receive lymph from efferent vessels
of the central axillary lymph nodes, therefore from all axillary lymph
node groups. The apical axillary nodes also receive lymph from those
lymphatic vessels accompanying the cephalic vein.
26. Efferent vessels from the apical axillary nodes travel through
the cervico-axillary canal, before converging to form the
subclavian lymphatic trunk.
The right subclavian trunk continues to form the right
lymphatic duct, and enters the right venous angle (junction of
internal jugular and subclavian veins) directly.
The left subclavian trunk drains directly into the thoracic duct.
27. LYMPHOEDEMA
• It is an abnormal swelling of limb due to the collection of excessive
amount of high protein fluid secondary to defective lymphatic
drainage in the presence of normal capillary filteration leading to
painful swelling of the extremity
• Lymphoedema affects around 2% of people and is common cause of
limb swelling.
• It is an abnormal accumulation of proteins in the body’s tissue (unlike
dependent edema).
• Over the period, lymphedema causes tissue proliferation of the affected
areas.
28. It leads to emotional and psychological distress affecting
relationships, education and work.
Difficulty in fitting garments (Tightening of Garments)
Patient feels emberrassed for seeking treatment.
Early diagnosis and treatment can prevent the development
of disabling late problems.
It is often misdiagnosed and mistreated by doctors thinking it
to be a cosmetic problem only .
29. Pathophysiology
Mechanical Insufficiency - lymphostatic
› Low-flow edema, low-volume insufficiency
› A breakdown in the transport capacity of the lymphatic
system
Dynamic Insufficiency - lymphodynamic
› High-flow edema, high-volume insufficiency
› A high load placed on the lymph system exceeds its
capacity
36. Classification
• Primary lymphoedema – Born with insufficient or
compromised lymphatic system, cause not known but
presumed to be due to ‘ congenital lymphatic dysplasia’.
• Secondary lymphoedema – May be a result of : Surgery
and/or radiation for cancer, Malignancy, Filariasis, Trauma,
Infection, Chronic Venous insufficiency or Obesity.
37. Aetiological
Classification
• Primary lymphoedema
• Congenital - onset <2 yrs
Sporadic
Familial (Milroy’s disease)
• Praecox (onset- 2 to 35yrs )
Sporadic
Familial (Meige’s disease)
• Tarda – onset – after 35 yrs
old )
• Secondary lymphoedema
• Parasitic – Filariasis
• Fungus -Tinea pedids.
• Exposure tosilica particles
• Primary lymphatic malignancy
• Lymph nodes metastasis
• Radiotherapy to L N
• Surgical excision of L N
• Trauma– Degloving injury
Sup.Thrombophlebitis, DVT.
41. Grade (Brunner) International Society of Lymphology (2013):
Subclinical - No apparent lymphoedema, Excess interstial fluid, Histopathological
changes in lymphatics and lymph nodes
Grade I - Pitting oedema,Swelling subsides on rest or elevation of extremity
Grade II - Oedema does not pit and does not reduce upon elevation
Grade III - Oedema associated with skin changes Iike fibrosis, excoriation.
Within each stage, severity based on volume excess as compared to the normal may
be sub-classified as minimal (<20% volume excess), moderate (20–40% volume
excess) or severe (>40%) volume excess.
42. To evaluate patients postoperatively and determine response to an
intervention a Volume Differential Reduction (VDR) is often calculated
Significant changes in BMI, not unusual in lymphedema patients, are
important to consider when assessing a patient’s limb volume change
over time. This is accounted for when applying the weight-adjusted
volume formula (WAC)
The volume excess when compared to the contralateral, unaffected,
limb or preferably to the same limb, prior to the onset of lymphedema,
when available is termed Volume differential (VD).
43. Stage IA: No clinical edema despite the presence of lymphatic dysfunction as demonstrated on
lymphoscintigraphy.
Stage IB: Mild edema that spontaneously regresses with elevation.
Stage II: Persistent edema that regresses only partially with elevation.
Stage III: Persistent, progressive edema; recurrent erysipeloid lymphangitis.
Stage IV: Fibrotic lymphedema with column limb.
Stage V: Elephantiasis with severe limb deformation, including scleroindurative pachydermitis and
widespread lymphostatic warts.
Campisi further correlated stage of lymphedema with amount of volume excess:
Stage I: 0–20% volume excess.
Stage II: 21–40% volume excess.
Stage III: 41–60% volume excess.
Stage IV/V: >61% volume excess.
Campisi et al. has described a staging system that uses clinical presentation
and lymphoscintigraphic patterns to help classify lymphedema and assist
with clinical management.
44. Chang et al. has devised a classification scheme using ICG
lymphangiography to assist with surgical planning in lymphedema of
the arm
Stage I: Many patent lymphatic vessels, with minimal, patchy dermal backflow.
Stage II: Moderate number of patent lymphatic vessels, with segmental dermal
backflow.
Stage III: Few patent lymphatic vessels, with extensive dermal backflow involving the
entire arm.
Stage IV: No patent lymphatic vessels seen, with severe dermal backflow involving the
entire arm and extending to the dorsum of the hand.
45. Conditionsmimicking
lymphoedema
• Factitious lymphoedema - Caused by application of a tourniquet (a start
and sharp cut off is seen on examination) or hysterical disuse of limb in
pts with psychological or psychiatric problems.
• Immobility lymphoedema - Generalised or localised immobility of any cause
leads to chronic limb swellling e.g-elderly person who spendsall day or night
sitting in a chair (arm chair legs ), the hemiplegic stroke patient or young
patient with multiple sclerosis.
• Lipoedema - Seen only in women as B/L symmetrical enlargement of legs
and sometimes lower half of the body due to abnormal
deposition of fat. It may or may not be associated with obesity .It can coexist
with other causes of limb swelling.
46. Differential
Diagnosis
• Non vascular or non lymphatics - General disease states - Liver
failure, Hypoproteinemia, CHF, Hypothyroidism, Allergic
(Angioedema), Prolonged Immobilization.
* Local disease processes – Arthritis, Haemarthrosis, Bony (or)
soft tissue tumours, Calf mucle hematoma.
* Retroperitoneal fibrosis
* Drugs – Steroids, Oestrogens, MAO inhibitors.
* Trauma * Obesity * Gigantism
50. Investigating Lymphoedema
• Are investigations necessary ?
• It is usually possible to diagnose and manage lymphoedema
purely on the basis of history and examination when swelling
is mild and there are nocomplicating features
• In pts with severe, atypical and multifactorial swelling
investigations may help to confirm the diagnosis management
and prognostic information.
51. Diagnosis
Clinical Examination
Circumferential Measurements.
Tissue tonometry
Perometry
Dermal backflow assessment
Bioimpedance spectroscopy (BIS) (L-Dex)
Diagnostic thresholds for upper limb LE - most commonly used thresholds
include: an absolute 200 ml inter-limb volume difference, a 2-cm inter-limb
circumference difference, a 5-cm inter-limb difference of the sum of all
circumference measurements or a relative percentage difference, often 10%
52. Investigations
• Routine Tests - TLC,DLC RFT, LFT, Thyroid function tests, total plasma
proeins, albumen, fasting blood sugar, urine exam for chyluria, blood
smear for microfilariae, X ray chest and ultrasound.
• Lymphangiography- Indocyanine green (ICG) lymphangiography) – Direct
method involves injection of contrast medium into peripheral lymphatic channel
followed by radiographic visualisation of the lymphatic vessels and nodes. It is the
gold standard for showing abnormalities of large lymphatics and lymph nodes. It
can be technically difficult , is unpleasant for the pt, may cause further injury to
lymphatics. As a routine it has become obsolete. Indirect lymphangiography
involves intradermal inj. Of water soluble non ionic contrast into a web space it is
taken up by lymphatics and is followed radiographically. It will show distal
lymphatics but not proximal lymphatics and lymph nodes.
53. • Isotope lymphoscintigraphy - This has become primary diagnostic technique
incase of unccertainty. Radioactive technitium labelled protein or colloid particles
are injected into interdigital web space and taken up by lymphatics. Serial films
are taken by a gamma camera. It provides a qualitative measure of lymphatic
function. Quantitative function is performed using adynamic (exercise) component
and specifically examines the anatomy and morphology of the lymphatic system.
It also provides information on lymphatic transport.
Based on lymphoscintigraphy-Lymphatic transport
index
TI = 0 optimal flow
TI =45 no flow
<10 normal
54. • Computed tomography - A single axial CT slice through the midcalf is a
useful test for lymphoedema (coarse, non enhancing reticular
honeycomb pattern in an enlarged subcutaneous compartment),
Venous oedema (increased volume of the muscular compartment and
lipoedema (increased sub cutaneous fat). CT will diagnose a pelvic or
abdominal mass lesion.
55. Investigation
s
• MRI – It can provide clear images of lymphatic channels and lymph nodes
and is useful in assessment of lymphatic hyperplasis, MRI scan differentiate
between venous and lymphatic causes of a swollen limb and can detect
tumours causing lymphatic obstruction
• HR Ultrasound - It can provide information about venous function like
DVT and venous abnormalities
• Pathological examination - If malignancy is suspected FNAC , neddle
cone biopsy or surgical excision from lymph nodes is useful. Skin biopsy will
confirm the diagnosis of lymphangiosarcoma.
56.
57.
58. Management – Conservative
Complex Decongestive Therapy (CDT)
• Skin care to treat infections (nail – fungal) and optimise condition of the
skin (skin – cellulitis) + Patient Education.
• Manual Lymphatic Drainage (MLD) to enhance lymph flow.This precedes bandaging
and directs lymph fluid to functional territories and helps to form collateral pathways
• Multi Layer Compression Bandaging
• Exercise to increase lymphatic & venous flow- Massage and swimming are
beneficial. Avoid vigrous exercises.
• A compressive garment therapy is used to preserve the reduction acieved by
treatment and prevent progression of lymphoedema Education and Psychosocial
support.
61. Manual Lymphatic Drainage (MLD)
• Increase lymphatic uptake
• Increase lymph vessel pulsation
• Promotes movement of fluid from edematous areas to
regions of normal lymphatic drainage
• Promotes relaxation
• Analgesic effect
Goals of technique:
1. Increase peristalsis of lymphangion
2. Break down fibrotic tissues
3. Increase lymph volume in lymph
vessels
4. Decrease congestion in interstitium
62. Treatment begins proximal, to “clear” proximal lymphotomes before
moving to affected lymphotomes
Massage is directed towards the cleared lymphotome
Pressure is very light
Strokes are rhythmic
Massaging lymph nodes
› Firmer pressure, circular motion
“Clearing”
› Begin farthest from the affected area
› Clears the way for fluid drainage
› Moves proximal to distal
63. “Flowing”
› Begin closest to the affected area
› Always done after clearing
› Moves distal to proximal
64. Medical Compression
Bandaging
Low stretch bandages
› Provides low stretch when no contraction
› Higher compression when muscles contract
Prevent re-fill of lymphatics
Work with muscle pumping
Follow “Law of Laplace” – the smaller the radius the greater the pressure
Help break up fibrotic areas
65. Bandaging Guidelines
Worn 23 hrs/ day (off only for bathing)
Should re-wrap daily to prevent loosening
Should have more compression (more layers) distally
Bandages should be washed frequently
66. Compression Therapy
Use of compression garments is very important in treatment of
lymphoedema - maintains reduction gained during therapy
-Transition to garments when reduction plateaus.
-They apply medically proper pressure to the swollen region to reduce
pooling of fluid.
These garments are available in a variety of styles, sizes, colours and
grades of compression (Class I- IV).
More swelling needs stronger support. They come as Pre–sized (ready to
wear) or custom made design. They are worn during day and removed at
night.
67. Therapeutic Exercises
Exercises facilitate muscle pumping
Should be done with compression
Progress proximally to distally
Very low resistance, few repetitions, rests as needed
69. Goals of surgical therpay
Improve function
Prevent further complications
Facilitate conservative therapy
Indications : failed medical management.
size is impairing normal function.
Relative : cosmetic .
Recurrent lymphangitis.
10 year conversion rate into lymphosarcoma is 10
%
70. AIM OF SURGERY
Reduce swelling
By pass lymphatic blockage
71. Surgical Management
Early 1990s
Early methods of managing lymphedema surgically involved
using a silk suture that was threaded in a subcutaneous plane
along the affected extremity.
72. lymphangioplasty
Handley
Introduced silk thread across lymphatic barrier
Capillary action drain fluid
But later dense fibrosis around thread prevents
capillary action
Proposed improvement : Teflon thread &
steroid injection
73. Suami and Chang classified the surgical management
- Ablative
- Physiologic
74. Ablative Surgery
In Ablative surgery - The soft tissues, which are edematous and fibrotic,
above the level of the deep fascia, are surgically removed with either
direct excision or by liposuction.
Aim at surgical removal of the tissue layers affected by lymphedema, the
deep fat compartment above the deep fascia, the superficial fat
compartment above the superficial fascia and below the dermis, and to
varying degrees the skin itself.
75. Ablation surgery
Basis : reduce lymph producing tissue
Sistrunk : removal of ellipses of skin and subcutaneous
tissue with primary closure
Homans : Staged excision of subcut tissue under flaps.
Charles : radical excision with STSG
Gibson : radical excision with FTG
Teimourian : lipectomy
Jaju : arterial ligation
76. Thompson et al. utilized modifications of Homan technique for the upper
extremity.
These modifications include excising affected tissue, then creating de-
epithelialized dermal flaps and folding these in toward, and suturing them to
the deep investing fascia,
- postulating that these dermal bridges would act as connections between
deeper lymphatics and vessels and superficial lymphatics facilitating fluid
transport.
There is no evidence to support that this takes place.
92 % of 72 cases of thompson improved
No e/o communication between dermal and muscle lymphatics
Improvement was attributed to excision
77. More recently, suction-assisted lipectomy / liposuction has been utilized as
an ablative method to remove the hypertrophied fat of the affected extremity.
- Much less morbid.
- No skin grafting is involved .
- External scarring at surgical sites is minimal.
Compression garments or wraps must be worn throughout the day following
liposuction to continue to control the excess fluid component and maintain
the volume reduction that was achieved
78. Currently, all these ablative methods should be reserved for more
advanced lymphedema that has undergone architectural changes in the
soft tissue and would thus be unresponsive to physiologic methods of
intervention.
79. Currently, most practitioners - combining physiologic procedures and
liposuction – in later stages of lymphedema with significant amounts of fat
hypertrophy and/or fibrosis.
Most physiologic methods - used for secondary lymphedema.
80. Physiological Surgery
Physiologic methods are those that recreate normal or alternate route for
lymph fluid to flow out of the affected limb.
Two main physiologic interventions are currently employed to treat
lymphedema.
1) Based on the creation of shunts between the congested lymphatic
channels and the venous system proximal to the site of lymphatic
obstruction.
2) Relies on the introduction of vascularized soft tissue flaps which
frequently include vascularized lymph nodes to the affected extremity
81. Jackobsen and Suarez - Lymphaticolymphatic bypass
Olszewski : Lymphnodovenous
O’brine : lymphaticovenous
Vascularized lymph node transfer (VLNT)
Vascularized omental flap transfer.
Simultaneous microsurgery breast reconstruction and
vascularized lymph node transfer
82. First described by Jackobsen and Suarez in 1962.
Baumeister et al.- used health lymphatic grafts from the lower extremity as
a means of bypassing upper arm lymphatics into healthy neck lymphatics
across the scarred axilla.
Campisi et al - instead of using lymphatic vessels as graft conduits, vein
grafts from the thigh were used.
This helped alleviate potential disruption of the lymphatic system and the
risk of additional secondary lymphedema at the donor site
83. Microvascular
O’brine : lymphatic vessels in a lymphedematous limb are
connected to nearby small veins and venules using
microsurgical and super-microsurgical techniques min of 3
anastomoses needed
- proven results in post mastectomy lymphedema
Baumester’s technique bridging the lymphatic block with
autologous graft
Both are for localized blocks
84. Campisi - vein interposition graft between the
lymphatic vessel bundles above and below the site
of lymphatic blockage to bypass.
The ventromedial lymphatic bundle of the thigh
consists of about 16 lymphatic channels this region is
useful for harvesting.
knee and the inguinal region are avoided.
Lymphatic grafts can be harvested up to about 30 cm
in length.
85. Lymphatic - vein anastomosis
Lymphnodovenous anastmosis
Basis : normal lymphovenous shunts open in
lymphedema
Pulp of node is removed and subcapsular
sinus is sutured to the vein
Best result with dilated sinuses and with max
LN transfer
Indication : palpable LN
86. Lymphovenous Anastmosis
Indication : nonpalpable LN
Sedlacek - end-to-side
Yamada - end-to-end anastomosis
Better in hyperplastic forms - Because after
decompression chances of thrombosis increases in
them.
Degni designed a special needle to facilitate the
insertion of lymphatic vessels into veins.
87. Vascularized lymph node
transfer
Vascularized lymph node transfer is useful in reducing lymphedema. One of the
larger studies by Becker et al. evaluated 1500 patients with stage I, II, and III
lymphedema who had undergone vascularized lymph node transfer. The
minimum follow up was 3 years. Findings included a 98% subjective
improvement.
40% of patients with stage I and stage II lymphedema had significant
improvement and required no further conservative therapy. For patients
withstage III lymphedema, 95% had some improvement and 98% remained
infection free. However, the stage III patients still required conservative therapy
to help control edema in the limb.
One of the major drawbacks to lymph node transfers is the potential for
iatrogenic secondary lymphedema at the donor sites.
88. Vascularized omental flap
transfer
Because of the risk of donor site lymphedema, clinicians have
sought out other sources of vascularized lymphatic tissue.
The omentum’s function as lymphatic organ has been explored for
possible applications in lymphedema management.
Surgeons began using the omentum as a pedicled flap attached to
its gastroepiploic vascular supply to aid with lymphatic drainage in
upper extremity lymphedema
Results from this approach have yet to be fully validated, but early
reports show promising results similar to vascularized lymph node
transfers
89. Simultaneous microsurgery breast reconstruction and
vascularized lymph node transfer
Recently, the use of a combined abdominal and groin lymph
node flap has been utilized to treat lymphedema in the upper
extremity for patients who have undergone mastectomy and
axillary lymph node sampling and have developed refractory
lymphedema. Results from this approach are limited due to
the lack of data currently available, but some improvement
has been noted
90. The most commonly performed surgical procedures for
lymphedema are LVA and Free vascularized lymph node
transfer.
Lymphatic Microsurgical Preventative Healing Approach
(LYMPHA). This method, championed in Italy, utilizes
lymphovenous anastomoses of upper extremity lymphatics
at the time of the axillary node dissection to bypass any
severed arm lymphatics immediately.
91. Points to remember
Current practices dictate that conservative measure be utilized first when
patients are initially diagnosed with lymphedema.
Most surgeons recommend physiologic procedures for patients that have
stage II or early stage III lymphedema.
Becker et al., results from vascularized lymph node transfer suggested
that patients who had surgical interventions earlier in the course of their
disease had better outcomes.
Explain the patient the actual condition
Avoid false assurances
92. In breast cancer pts.
To avoid intravenous blood draws and intravenous catheter
placements in the at risk limb.
Avoid blood pressure measurements in the limb
Encourage Use of compression garments during air travel
are sometimes recommended.