2. Introduction
Cardiovascular disease responsible for 80% of mortality in diabetic
Studies provide evidence for specific cardiomyopathy contribute to
myocardial dysfunction in the absence of CAD
2
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
3. Definition of Diabetic cardiomyopathy
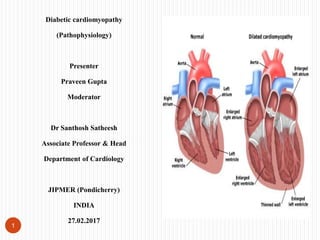
Characterized by myocardial dilatation
& hypertrophy
Decrease in systolic & diastolic
function
Independent of the coexistence of
ischemic heart disease or hypertension
Subclinical for long time
Hyperglycemia pathogenetic factor
3
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
4. DMCMP phenotype
In the restrictive/ heart failure with preserved
ejection fraction phenotype cardiomyocytes
are hypertrophied, collagen is laid down in-
between cardiomyocytes (reactive fibrosis)
(left-hand panel) and sarcomeric structure is
preserved (right hand panel).
In the dilated/ heart failure with reduced
ejection fraction phenotype, cardiomyocytes
are small and damaged, collagen is laid down
over larger areas (replacement fibrosis) (left-
hand panel) and sarcomeres have disappeared
(right hand panel)
Reproduced with permission from Van
Heerebeek et al.
4
6. Pathophysiological substrate of DCM
Anatomical damage of the myocardial
substrate
Atheroma more extensive, more
diffuse, and involves distal vessels in
coronary
Pathologic alterations of small
coronary vessels and the myocardial
endothelium include increased cell
adhesiveness, impaired relaxation,
impaired fibrinolysis, and increased
permability
Impaired myocardial contractility Inflammation in diabetic coronary arteries. A, Coronary
fibroatheromas illustrating the extent of macrophage (MΦ) and T
cells, (CD45RO) and HLA-DR expression in patients with type I and
II diabetes mellitus (DM) and nondiabetic subjects.
6 Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
7. Structural alterations leading to ventricular dysfunction
Medial layers of arterioles throughout the cardiac circulation show “hyaline” change, an
amorphous, ground glass appearance, resulting from breakdown of structural proteins
(largely thought to be collagen) and the uptake of glycated plasma proteins into the
vessel wall
Reduced blood supply resulting from microvascular disease and affecting vasa vasorum
in diabetes further damages small and medium arterioles of diabetic heart
7
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
8. Functional alterations of DCM
Impaired diastolic compliance and
maintenance of the systolic
function is usually the initial heart
lesion in the progression of DCM.
Failure of diastolic relaxation of the
left ventricle leads to impaired
filling and reduced cardiac reserve
on exercise
8
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
9. Molecular substrate of DCM
Hyperglycemia causes significant
functional alterations to the cellular
Na+–Ca2+ ionic channel
Decreased extrapolation and an
increased intracellular concentration of
ionic calcium
Dysfunction of cellular Na+–K+
channel
Increase in the intracellular sodium
Increase intracellular calcium in
cardiac myocytes
9
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
10. Cardiac autonomic neuropathy in DCM
Cause a reduction in the cardiac
ejection fraction,
Impair systolic dysfunction and
decrease diastolic filling
Deterioration of diastolic myocardial
function
10
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
11. Risk factors for DCM
Hyperglycemia
Formation of AGEs causing thickening
and leakage of the vasculature and
forming irreversible and abnormal
deposits of plasma-derived proteins in
the myocardial subintimal arterial
layers
Microvascular advanced glycation end-products deposition in diabetes
mellitus-related cardiomyopathy. AGEs, advanced glycation end-products.
Reproduced with permission from van Heerebeek et al
11
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
12. Risk factors for DCM
Hyperglycemia
AGEs generate toxic reactive
oxygen species (ROSs) that impair
cellular interactions and damage
myocardial vascular function,
causing endothelial vasomotor
dysfunction
12
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
13. Risk factors for DCM
Insulin resistance and the metabolic
syndrome
Hyperinsulinemia and insulin resistance
are also associated with a cluster of
thrombotic risk factors, such as elevated
levels of PAI-1, factor VII, factor XII,
and fibrinogen
13 Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
14. Risk factors for DCM
Dyslipidemia
Increased atherogenesis and insulin
resistance in diabetes and MetS
have been attributed in large part to
a proathero-thrombotic
dyslipidemia, related to
hypertriglyceridemia, elevated very
low-density lipoprotein, and
decreased HDL cholesterol levels
14
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
15. Risk factors for DCM
Hypertension
Pevalence of hypertension is
higher
Insulin resistance cause of
hypertension and DCM in type 2
15
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
16. Risk factors for DCM
Obesity
Reduced levels of adiponectin, an
insulin-sensitizing protein whose
secretion by adipose tissue is
paradoxically decreased in obesity,
may also contribute to insulin
resistance and DCM
16
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
17. Effect of diabetic nephropathy
Microalbuminuria is associated
with endothelial dysfunction,
abnormalities of the renin–
angiotensin system, and widespread
vascular basement membrane
defects
17
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.
18. Conclusion
Pathogenic contribution to the development of DCM includes
Insulin resistance
Increased formation of AGEs, MetS, hyperglycemia, dyslipidemia, obesity, and
presence of microangiopathy
Interplay is complex
Should be equally predicted and effectively treated
18
Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes
to current diagnosis and management strategies. Vascular health and risk management. 2010 Oct 21;6(1):883-903.