1. Hospital readmissions are a significant current focus of healthcare
organizations and payor sources with significant resources being
devoted to readmission prevention. Current literature shows mixed
results for different programs targeting readmission rates. Post-
hospitalization home visits represent a potential intervention for
improving care transitions and reducing readmissions.
Outcomes of a home visit
transitional care model to
reduce hospital admission for
high-risk patients
Background
● Accurately identify patients at high risk for readmission
Reduce hospital readmission and unnecessary ED use by
making in-home patient visits using mid-level providers
Reduce cost to the healthcare system and improve the overall
health and satisfaction of the target population
Develop the technology infrastructure that will direct multiple
providers making home visits in the most cost-effective, time-
efficient manner possible
●
●
●
Goals
In 2013, WakeMed Health and Hospitals in Raleigh, NC, partnered with
Paired Health, a health-services and technology company, to provide
post-hospitalization transitional care home visits. Referrals were made
by discharging physicians and case managers. Providers could refer
anyone they felt were at high-risk for readmission, but referrals were
encouraged for patients with repeat hospitalizations and emergency
room visits, patients without primary care physicians and patients who
had missed post-discharge follow-up after prior admissions. Patients
were followed for up to 30-days, or until care was assumed by a primary
care physician, whichever occurred first. We reviewed the 30-day
readmission rates to WakeMed for these patients during the program's
first year of implementation. This was compared to the hospital's overall
Medicare readmission rate to WakeMed during that same period.
Program Description
Have at least one complex illness, multiple
comorbidities and psychosocial problems
Have multiple risk factors that could
push them into high-risk/high-cost
category if unaddressed
Healthy or have well-managed
chronic conditions
Identify high-risk patients
Case managers and discharging MD’s
Rapid online referral
Identify evidence-based risk factors
Clinical assessment
Stratification tool (based on BOOST 8 P’s)
Provider availability and patient location
Disease-specific clinician
Most efficient and cost-effective route
Evidence-based templates to direct provider
assessment and treatment plan
Care plans determine timing and frequency of
home visits
Patient Navigator
Communicate and provide content of home
encounters
Mike Watson, M.D., Michael Craig, M.D.
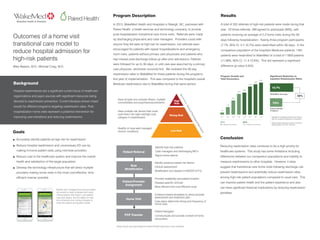
A total of 332 referrals of high-risk patients were made during that
year. Of those referrals, 299 agreed to participate (90%), with
patients receiving an average of 2.2 home visits during the 30-
days following hospitalization. Twenty-three program participants
(7.7%; 95% CI, 4.7-10.7%) were readmitted within 30-days. In the
comparison population of the hospital's Medicare patients, 1491
patients were readmitted to WakeMed of a total of 11859 patients
(11.98%; 95% CI, 11.4-12.6%). This did represent a significant
difference (p-value 0.024).
Results
WakeMed FY12 Medicare Readmission Rate for
high-risk hospital discharges as a comparative
Patient Referral
Risk
Stratification
Patient/Provider
Assignment
Home Visit
PCP Transfer
Steps above are automated by Paired Health application and software
Mobile care management tools provided:
(a) access to daily schedule and route,
clinical patient information, and patient
care plan status; and (b) ability for real-
time schedule and routing changes to
meet the patient and system needs
Reducing readmission rates continues to be a high-priority for
healthcare systems. This study has some limitations including
differences between our comparison populations and inability to
measure readmissions to other hospitals. However, it does
suggest that transitional care home visits following discharge can
prevent readmissions and potentially reduce readmission rates
among high-risk patient populations compared to usual care. This
can improve patient health and the patient experience and also
can have significant financial implications by reducing readmission
penalties.
Conclusion
Program Growth and
Total Encounters
2013 2014
883 Patient Encounters 2,217 Patient Encounters
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
42
153
281
407
435435
553
597
632
Significant Reduction in
Inpatient Readmission Rates
30-day inpatient readmission rate for the Paired
Health program (Q1 2013 - Q3 2014)
1
2
WakeMed Average
Paired Health
Program
7.6%
14.7%
1
2
48%
High
Risk
Rising Risk
Low Risk
Clinical&PsychologicalRiskFactors