Cranial Hemorrhage of The Newborn
•Télécharger en tant que PPTX, PDF•
3 j'aime•560 vues

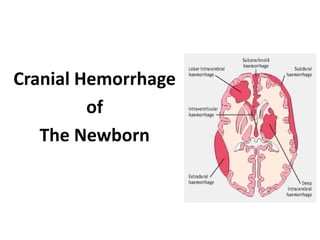
Cranial hemorrhage in newborns can be extracranial (e.g. cephalhematoma) or intracranial (e.g. subdural hemorrhage). Intracerebral hemorrhage, especially germinal matrix and intraventricular hemorrhage, is the most common type seen in preterm infants. Risk factors include prematurity, fluctuations in blood pressure, and hypoxic events. Intraventricular hemorrhage is graded based on its extent using cranial ultrasound or CT scan. Most hemorrhages occur within 3 days of birth and management involves supportive care though progressive ventricular dilation may require ventricular shunting. Outcomes depend on the grade of hemorrhage

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Cranial Hemorrhage of The Newborn
Similaire à Cranial Hemorrhage of The Newborn (20)
Plus de Syed Kamrul Hasan
Plus de Syed Kamrul Hasan (16)
Dernier
Dernier (20)
Cranial Hemorrhage of The Newborn
- 2. Contents Introduction Classification Etiology Risk factors Pathophysiology Clinical feather Approach of diagnosis Spread of hemorrhage Timing of hemorrhage Management of IVH prognosis
- 3. Central Nervous System Disorders are important cause of neonatal mortality & both short & long term morbidity. The CNS can be damaged as a result of asphyxia, hemorrhage, trauma, hypoglycemia or direct toxicity. Traumatic hemorrhage may involve any layer of the scalp as well as intracranial contents.
- 4. Classification Cranial Hemorrhage Intracranial Hemorrhage Extra cranial Hemorrhage • Cephalhaematoma • Caput succedaneum • Subgaleal haemorrhage • Retinal & sub conjunctival haemorrhage • GM hemorrhage • Subdural hemorrhage • Epidural hemorrhage • Subarachnoid hemorrhage • Intracerebral hemorrhage • Intracecrebellar hemorrhage
- 6. Caput Succedaneum Subcutaneous fluid collection in the soft tissue of the scalp that is presented during vertex delivery.
- 7. Cephalhaematoma • Sub periosteal collection of blood which does not cross the suture line. • Presents as a soft , fluctuant mass usually over the parital bone.
- 8. Sub Galeal Hemorrhage • Hemorrhage between galea aponeurotica of scalp & the periosteal. • It appears as a fluctuant mass within few hours after birth & can extend from the orbital ridge to the nape of neck & laterally to the ears crossing the suture line.
- 9. Sub Conjunctival & Retinal Hemorrhage • These are frequent ; petechiae of the skin of the head & neck are also common. • These hemorrhages are temporary & the result of the normal vaginal delivery. • These lesion resolves rapidly within the 1st two weeks of life.
- 11. Intra Cranial Hemorrhages • Traumatic epidural, subdural or subarachnoid hemorrhage is specially likely when the fetal head is large in proportion to the size of the mothers pelvic outlet, with prolong labor, in breach presentation or as a result of mechanical assistance with delivery. • The majority of subdural & subarachnoid hemorrhages resolves without intervention.
- 12. Subdural Hemorrhage • A sub dural haemorrhage (SDH)is an accmulation of blood between the dura & arachnoid mater. • SDH is very common after birth : upto 50% of term asymptomatic infants may have SDH.only on rare ocassions does SDH become serious. • Symptomatic subdural hemorrhage in large term infants should be treated by removal of the subdural fluid collection with a needle placed through the lateral margin of the anterior fontanel. • Asymptomatic subdural hemorrhage following labour should resolve by 4 weeks of age.
- 13. Epidural Hemorrhage Blood between the inner skull & dura mater. It is extremely rare in newborn infants. In case of epidural hemorrhage, removal or aspiration of the hemorrhage was performed in the majority of the cases, and the prognosis was quite good except when other Intracerebral or parenchymal pathology was absent.
- 14. Subarachnoid Hemorrhage • Subarachnoid hemorrhage(SAH) is an accumulation of blood between the arachnoid mater & pia mater. • Subarachnoid hemorrhage is rare & typically silent. • Some infants experience seizure on the 2nd day of life. • Rarely infants has a life threatening catastrophic hemorrhage & dies. • There are usually no neurologic abnormalities during the acute episode or on follow-up.
- 15. Intracerebral Intraparenchymal Hemorrhage • It occurs deep within the brain tissue after venous infarction & is commonly referred to as periventricular hemorrhagic infarction(PVHI). • Occurrence of PHHI may be as much as 10 - 15% among infants with ICH.
- 16. Intracerebellar Parenchymal Hemorrhage(ICPH) • ICPH is most often seen in preterm infants with complications of labor & delivery. • Using cranial USG 2.8% <1500gms 8.7% <750gms • Using MRI infants <34 weeks of gestation it is 10%.
- 17. Germinal Matrix & Intraventricular Hemorrhage(IVH) IVH is the most common CNS complications of a preterm birth. the occurrence is greatly associated with the immaturity of the germinal matrix of the lateral ventricles.
- 18. Etiology • The over all incidence has decreased over the past decades as a result of improved perinatal care. • Incidence & severity is inversely proportional to the gestational age & birth weight.
- 19. Etiology • 30% premature infants < 1500 grams may develop IVH. • 7% of 1 kg to 1.5 kg( grade 3 or 4) • 14% of 751 to 1000gms • 24% of < 750 grams may develop severe IVH(grade 3 or 4) • 3% of infants <1000gms develop periventricular leukomalacia.
- 20. 1) Prematurity is the most important risk factor for IVH. 2) Rapid volume expansion 3) Hypertension 4) Coagulopathies 5) Hypoxic-ischemic insults 6) Respiratory disturbances 7) Acidosis 8) Infusions of hypertonic solutions 9) Anemia 10) Vacuum-assisted delivery 11) Frequent handling 12) Tracheal suctioning Risk Factors
- 21. Germinal Matrix • Primitive cellular region ventrolateral to LV prominent : 26-34 involute : term • Contains pluripotential migrating cells neurons, astrocytes, oligodendroglia • Contains immature blood vessels thin walls(lack muscularis layer) immature cell junction & basal lamina
- 22. Pathogenesis • IVH in preterm occurs in sub ependymal germinal matrix. • This is located between caudate nucleus and the ependymal lining of the lateral ventricle. • This area is site of origin of embryonal neurons and fetal glial cells. • This area is highly vascularized and weakly supported. • The blood vessels in this area are immature and are prone to hypoxic ischemic injury.
- 23. Pathogenesis • Fluctuation in cerebral blood flow play an important role in developing IVH. • A sudden rise in systemic blood pressure may result in an increase in cerebral circulation with subsequent rupture of the germinal matrix vessels. • Decreases in cerebral blood flow can result in ischemic injury to germinal matrix vessels, which rupture on reperfusion.
- 24. Clinical Feature Three types of presentations 1. Catastrophic Deterioration – least common, evolution over minutes to hours. marked detorioration of sensorium, aponea, seizures, pupil fixed to light, eye fixed to vestibular stimulation, decrebration & flacid quadriparesis. 2. Saltatory detorioration – evolution over hours to days. alteration in sensorium, hypotonia, decreased spontaneous movement, abnormal eye position or movement, bulging fonanelle.
- 25. Clinical Feature 3. Clinically Silent – most common. usually occur with smaller lesion. there can be associated signs of blood loss such as pallor, shock, decreased haematochrit, metabolic acidosis, jaundice.
- 26. Approach of Diagnosis History Clinical Manifestations CT scanCranial Ultrasonography
- 27. • The clinical signs of IVH are non specific, so therefore, it is recommended that cranial ultrasound should be done in premature infants <32 week of gestation . • Infants <1000g are at highest risk and should undergo cranial ultrasonography within, first 3-7 days of age after birth. Approach of Diagnosis
- 28. Volpe’s grading(CUS) Severity Description 1 GMH with no or minimal IHV(<10% of ventricular volume) 2 IVH occupying 10-50% of ventricular area 3 IVH occupying >50% of ventricular area 4 Periventricular echodensity
- 29. Papile’s grading(CT) Severity Description 1 Isolated GMH 2 IVH without ventricular dilatation 3 IVH with ventricular dilatation 4 IVH with parenchymal hemorrhage
- 37. Spread of Hemorrhage • 40% stays in GM( grade1) • 60% enters ventricles (grade 2& grade 3) large IVH obstructs CSF flow rapidly progressive hydrocephalus small IVH retards CSF absorption slow evolving hydrocephalus • PV hemorrhagic infarction (grade 4)
- 38. Timing of IVH • 90% occurs within first 72 hours 50% : < 24 hours 25% : >24 & <48hours 15% : >48 & < 72 hours • 20% - 40% progress further maximal extension occurs 3 – 5 days after initial insult.
- 39. Management of Intraventricular hemorrhage Prevention Acute Management Follow up Post natal prevention Antenatal prevention
- 40. • Avoid preterm delivery • Antenatal phenobarbital, vit K, & magnesium sulfate have not been conclusively demonstrated to prevent IVH. • C section of high risk deliveries. • A single course of antenatal corticosteroids is recommended in pregnancies 24-34 weeks of gestation that are at risk for preterm delivery. Antenatal Prevention
- 41. • Avoid birth asphyxia. • Avoid large fluctuation in blood pressure. • Avoid excessive handling. • Avoid rapid infusion of volume expander or hypertonic solutions. • Correct acid base balance. • Correct coagulation abnormalities. • Prophylactic administration of low dose indomethacin (0.1mglkglday) for 3 days, reduces the incidences of severe IVH. Postnatal Prevention
- 42. Management of IVH • No specific management is available for IVH, it may be associated with other complications that require therapy. • ABC management. • Seizures are treated aggressively with anticonvulsant drugs.
- 43. Management of IVH • Anemia & coagulopathies requires transfusion with packed red blood cells or fresh frozen plasma. • Shock & acidosis are treated with slow administration of sodium bicarbonate & fluid resuscitation.
- 44. Management of IVH • Insertion of VP shunt is the preferred method to treat progressive & symptomatic PPH. • Serial lumber punctures, ventricular taps or reservoirs & externalized ventricular drains are potential temporizing interventions.
- 45. No further treatment No therapy, close observation for 1 yrs VP shunt or VSG shunt No further treatment, observe for 1 yr Slowly progressive ventricular dilation Close surveillance for 2-4 weeks Continued dilation Serial LP or placement of ventricular drainage device,+/- medication Continued dilation Stop dilation No PVD Rapidly progressive ventricular dilation Monitor OFC & fontanelle daily, serial CUS(2-7) days to asses ventricle size,shape & RI Serial LP every 1-3 days , depending on rate of ventricular dilation Continued dilation Dilation stops
- 46. Prognosis Grade of GM- IVH Mortality rate(%) Progressive ventricular dilatation(% of survivors) Incidence of definitive neurological sequlae(% of survivors) 1 5 5 15 2 10 20 25 3 20 55 50 4 50 80 75
- 47. References • Nelson Textbook of Pediatrics • Neonatology (Tricia Lacy Gomella) • Manual of Neonatal Care (John P. cloherty, Eric C .Eichenwald , Ann R Stark)