Transposition of the great arteries
•Télécharger en tant que PPT, PDF•
9 j'aime•7,893 vues

Transposition of the great arteries is a serious but rare heart defect present at birth (congenital), in which the two main arteries leaving the heart are reversed (transposed). The condition is also called dextro-transposition of the great arteries.

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Transposition of the great arteries
Similaire à Transposition of the great arteries (20)
Plus de jagan _jaggi
Plus de jagan _jaggi (20)
Dernier
Dernier (20)
Transposition of the great arteries
- 1. TRANSPOSITION OF THE GREAT ARTERIES ATRENDYNURSE
- 2. INTRODUCTION Transposition of the great arteries is a congenital (present at birth) heart defect. Due to abnormal development of the fetal heart during the first 8 weeks of pregnancy, the large vessels that take blood away from the heart to the lungs, or to the body, are improperly connected.
- 4. Transposition of the Great Arteries Most common form of cyanotic congenital heart disease (5 to 7% of all congenital heart defects ) which presents in the newborn period. More common in males Babies are usually normal birth weight and size. 1. Aorta emerges from RV 5. PDA 2. PA emerges from LV 3. VSD 4. ASD
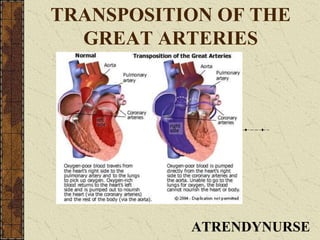
- 5. In transposition of the great arteries, the aorta is connected to the right ventricle, and the pulmonary artery is connected to the left ventricle - the exact opposite of a normal heart's anatomy. Oxygen-poor (blue) blood returns to the right atrium from the body, passes through the right atrium and ventricle, then goes into the misconnected aorta back to the body. Oxygen-rich (red) blood returns to the left atrium from the lungs, passes through the left atrium and ventricle, then goes into the pulmonary artery and back to the lungs.
- 6. Two separate circuits are formed - one that circulates oxygen-poor (blue) blood from the body back to the body, and another that recirculates oxygen-rich (red) blood from the lungs back to the lungs. Because of the low amount of oxygen provided to the body, TGA is a heart problem that is labeled "blue-baby syndrome.“ Associated heart abnormalities: they actually may be necessary in order for an infant with transposition of the great arteries to live. Ventricular septal defect – the most common Left ventricular outflow tract obstruction. Atrial septal defect Patent ductus arteriosus
- 7. CAUSES: Some congenital heart defects may have a genetic link, either occurring due to a defect in a gene, a chromosome abnormality, or environmental exposure, causing heart problems to occur more often in certain families. Most of the time this heart defect occurs sporadically (by chance), with no clear reason for its development.
- 8. Physical Findings: Indication of TGA is a newborn who becomes cyanotic (blue) in the transitional first day of life when the maternal source of oxygen (from the placenta) is removed. Cyanosis is noted in the first hours of life in about half of the infants with TGA, and within the first days of life in 90 percent of them. The degree of cyanosis is related to the presence of other defects that allow blood to mix, including a PDA- cyanosis, seen in lips and under fingernail beds – may not be present.
- 9. Physical Findings: Congestive heart failure will develop because of the extra blood flow going to the lungs. Consistent with CHF = there is poor feeding, poor weight gain, sweating, and fast or labored breathing, rapid heart rate ,cool, clammy skin Cyanosis will not improve with the application of oxygen – if it does, then the problem is pulmonary, not cardiac. The second heart sound is loud and single heart murmur, depending if there is a VSD or not
- 10. WHY IS TRANSPOSITION OF THE GREAT ARTERIES A CONCERN? The right ventricle, connected to the aorta in TGA, is the weaker of the two ventricles. Because the right ventricle is weaker, it may not be able to pump blood efficiently to the body, and it will enlarge under the strain of the job. The left ventricle may pump blood into the lungs more vigorously than needed, leading to strain in the blood vessels in the lungs.
- 11. History & Physical findings chest x-ray electrocardiogram (ECG or EKG) echocardiogram (echo) , if not 100% definitive Cardiac Cath cardiac catheterization - gives very detailed information about the structures inside the heart. Under sedation, a small, thin, flexible tube (catheter) is inserted into a blood vessel in the groin, and guided to the inside of the heart. Blood pressure and oxygen measurements are taken in the four chambers of the heart, as well as the pulmonary artery and aorta. Contrast dye is also injected to more clearly visualize the structures inside the heart. DIAGNOSIS:
- 12. TREATMENT BASED ON: Child's age, overall health, and medical history Extent of the disease Child's tolerance for specific medications, procedures, or therapies Expectations for the course of the disease Opinion or preference of parents Combination of defects that accompany the primary problem of TGA. Development of early pulmonary vascular disease is also common. The changes associated with PVD can occur as early as a few weeks of life and tend to occur more frequently in babies who have ventricular septal defects in addition to TGA. Early corrective surgery minimizes the chances of development of PVD.
- 13. 1)As part of the cardiac catheterization, a procedure called BALLOON ATRIAL SEPTOSTOMY may be performed to improve mixing of oxygen-rich (red) and oxygen-poor (blue) blood. BALLOON ATRIAL SEPTOSTOMY A special catheter with a balloon in the tip is used to create an opening in the atrial septum (wall between the left and right atria). The catheter is guided through foramen ovale (a small opening present in the atrial septum that closes shortly after birth) and into left atrium.The balloon is inflated. The catheter is quickly pulled back through the hole, into the right atrium, enlarging the hole, allowing blood to mix between the atria. TREATMENT
- 14. BALLOON ATRIAL SEPTOSTOMY A special catheter with a balloon in the tip is used to create an opening in the atrial septum (wall between the left and right atria). The catheter is guided through the foramen ovale (a small opening present in the atrial septum that closes shortly after birth) and into the left atrium. The balloon is inflated. The catheter is quickly pulled back through the hole, into the right atrium, enlarging the hole, allowing blood to mix between the atria. 2) PROSTAGLANDIN E1 :An intravenous medication called prostaglandin E1 is given to keep the ductus arteriosus from closing.
- 16. SURGICAL PROCEDURES: ARTERIAL SWITCH: • The aorta and pulmonary artery are divided and reconnected so that the pulmonary artery is connected to the right ventricle and supplies deoxygenated blood to the lungs. • The aorta is connected to the left ventricle and supplies oxygenated blood to the body. • The coronary arteries are also relocated so that they will receive oxygenated blood from the aorta. • Any septal defects are closed at the same time
- 17. Transposition of the Great Arteries
- 18. MUSTARD OR SENNING OPERATION If the baby is older at the time of diagnosis or there is an unusual location of one of the coronary arteries, the surgeon may choose to perform an atrial switch operation called a Mustard or Senning operation. For this operation the heart/lung bypass machine is used.The venous drainage of blood coming into the heart is rerouted rather switching the arteries that carry blood out of the heart. .
- 19. In this case : 1) the blue blood returning to the right atrium is redirected to the left atrium, flows to the left ventricle where it is pumped through the pulmonary arteries to the lungs. 2) Red blood returning from the lungs is baffled to the right atrium , flows to the right ventricle where it is pumped through the aorta and out to the body. Even though the blood goes to the right location, the heart remains configured so the right ventricle pumps blood to the body and the left ventricle pumps blood to the lungs MUSTARD OR SENNING OPERATION
- 20. Long-term complications of the Mustard procedure: Systemic heart failure Arrhythmias Venous return stasis Pulmonary edema Sudden death MUSTARD OR SENNING OPERATION
- 21. MUSTARD OR SENNING OPERATION
- 22. Transposition of the Great Arteries 1. Deoxygenated blood redirected to LA 2. LV Lungs 3. Oxygenated blood from lungs redirected to RA 4. RV Body
- 23. RASTELLI PROCEDURE: • Performed for TGA with left ventricular outflow obstruction • The ventricular septal defect is closed in such a way that the left ventricle is connected to the aorta and the right ventricle is connected to the lungs using a conduit with a valve in it. • One end of the conduit is connected to the right ventricle where blood exits into the pulmonary artery and the other end is attached to the pulmonary artery • The conduit acts a bypass around the naturally occurring narrowing. This conduit will need to be replaced as the child grows. Usually this is not necessary for 3 to 5 years after the original operation if done in infancy and then 1 to 2 more times throughout the child's life. SURGICAL PROCEDURES:
- 24. 1. VSD closed with patch 2. Conduit RASTELLI PROCEDURE:
- 25. POSTOPERATIVE CARE FOR YOUR CHILD: After surgery, infants will return to the intensive care unit (ICU) for a few days to be closely monitored during recovery. While child is in the ICU, special equipment will be used to help him/her recover, and may include the following: ventilator –It breathes for the child while he/she is too sleepy to breathe effectively on his/her own. After surgery, children will benefit from remaining on the ventilator overnight or even longer so they can rest.
- 26. Centralvenous (IV) catheters - provide IV fluids and important medicines that help child recover from the operation. arterial line - measures blood pressure continuously during surgery and while child is in the ICU. nasogastric (NG) tube - keeps the stomach drained of acid and gas bubbles that may build up during surgery. urinary catheter - drain out of the bladder and accurately measures how much urine the body makes, which helps determine how well the heart is functioning. chest tube – heart monitor - POSTOPERATIVE CARE FOR YOUR CHILD:
- 27. After surgery, the heart will be a little weaker than it was before, and, therefore, the body may start to hold onto fluid, causing swelling and puffiness. Diuretics may be given to help the kidneys to remove excess fluid from the body. Some infants are just tired, and need to build their strength up before they will be able to learn to bottle feed. Strategies include : high-calorie formula or breast milk Special nutritional supplements may be added to formula or pumped breast milk that increase the number of calories in each ounce, thereby allowing your baby to drink less and still consume enough calories to grow properly. supplemental tube feedings that can either supplement or take the place of bottle-feedings. Infants too tired - feeding tube alone. POSTOPERATIVE CARE FOR YOUR CHILD:
- 28. Long-term outlook after TGA surgical repair: Many infants who undergo TGA surgical repair will grow and develop normally. However, after TGA repair, infant will need to be followed periodically by a pediatric cardiologist who will make assessments to check for any heart-related problems, which include : fast, slow, or irregular heart rhythms leaky heart valves narrowing of one or both of the great arteries at the switch connection site(s) narrowing of the coronary arteries at their switch connection site
- 29. THANK YOU