Extraocular Muscles: Anatomy
•Télécharger en tant que PPTX, PDF•
2 j'aime•723 vues

Extraocular Muscles: Anatomy

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Extraocular Muscles: Anatomy
Similaire à Extraocular Muscles: Anatomy (20)
Plus de Mero Eye
Plus de Mero Eye (20)
Dernier
Dernier (20)
Extraocular Muscles: Anatomy
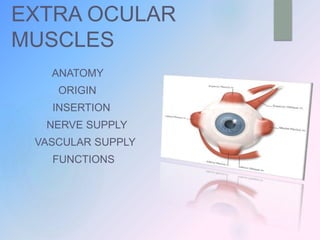
- 1. EXTRA OCULAR MUSCLES ANATOMY ORIGIN INSERTION NERVE SUPPLY VASCULAR SUPPLY FUNCTIONS
- 2. DISCUSSION AREAS EMBRYOLOGY ANATOMY ORIGIN COURSE INSERTION NERVE SUPPLY BLOOD SUPPLY FUNCTIONS Clinical significances
- 3. EMBRYOLOGY EOMs (4 recti & 2 oblique) differentiate from the mesenchyme in the region of developing eyeball (prechordal mesenchyme) Originally represented as a single mass of mesenchyme, they later separate into distinct muscles
- 4. appear approximately in the following sequences : SR & LR → 5th week MR & SO → 6th week followed by IR & IO In the 8th week, all the motor nerves of the eye reaches the EOMs.
- 5. EXTRA OCULAR MUSCLES RECTUS MUSCLES OBLIQUE MUSCLES Muscles responsible for the controlled movements of the eyeballs
- 7. ORIGIN a common tendinous ring ( the annulus of Zinn), attached at the apex of orbit SR & MR lie closely attached to the dural sheath of optic nerve at their origin
- 9. COURSE All the 4 recti run forward from their origin course is diverging ; however muscles converges slightly in front of the equator to get inserted on the sclera SR is separated from orbital roof by LPS muscle MR & LR follow the coresponding walls of orbit in most of the parts in their course IR follow the orbit for only about half its length
- 11. INSERTION Rectus muscles do not form a circle concentric with the limbus, rather form a spiral (the spiral of Tillaux) Fuchs (1884)
- 12. Duane Retraction Syndrome A congenital ocular motility defect due to fibrous tightening of lateral or medial rectus, or both Type I DRS : limitation of abduction Type II DRS : limitation of adduction Type III DRS : limitation of both adduction & abduction
- 14. “Retraction of globe & narrowing of palpebral fissure” on attempted adduction
- 15. Strabismus fixus A rare condition characterized by bilateral fixation of eyes in convergent position, due to fibrous tightening of medial recti
- 16. Strabismus fixus
- 17. OBLIQUE MUSCLES
- 18. SUPERIOR OBLIQUE MUSCLES arise from the bone (body of Sphenoid) above & medial to the optic foramen ORIGIN
- 19. COURSE SO muscle moves forward between the roof & medial wall of orbit to reach the trochlea, & turns postero-laterally to get inserted onto the sclera TROCHLEA : a thick fibrous cartilaginous pulley attached to spina trochlearis on the under aspect of frontal bone, at the superomedial angle
- 20. Reflected tendon of SO passes under the SR, & fans out to get inserted on to the sclera
- 21. INSERTION width of Insertion line : about 11mm (7-18 mm) Anterior end : lies 13.8mm behind the limbus Posterior end : lies 18.8mm behind the limbus
- 22. fact… Superior Oblique : longest & thinnest EOM length of its direct part : 40mm reflected tendon : 19.5 mm TOTAL : 59.5 mm
- 23. Brown’s SO Tendon Sheath Syndrome A congenital ocular motility defect due to fibrous tightening of SO tendon usually straight in primary position characterized by limitation of elevation of the eyes in adduction (normal elevation in abduction)
- 24. INFERIOR OBLIQUE MUSCLES arises by a rounded tendon from a shallow depression on the orbital plate of maxilla only muscle to originate from the front of orbit ORIGIN COURS E runs between IR & floor of orbit, laterally & backward
- 25. INSERTIO N It is inserted by a short tendon (1 to 2 mm long) in the lower & outer part of sclera behind the equator Near the insertion, Inferior Vortex vein is in relation to its posterior border shortest EOM → 37mm
- 26. Adhrence Syndromes a rare condition arises through abnormal fascial connections between the reflections of Tenon’s Capsule along the EOMs causing tethering of the globe
- 27. occurs between : IR& IO → limits elevation LR & IO → limits adduction SR & SO → limits depression
- 28. NERVE SUPPLY
- 29. supplied by Cranial Nerves (CN) CN III (oculomotor ) supplies IR SR MR IO
- 30. The branches from inferior division of CN III supply IR, MR & IO The branch for SR originate from the upper division of CN III
- 31. SO → supplied by CN IV (Trochlear nerve) the nerve divides into 3 or 4 branches LR → innervated by CN VI (Abducens nerve)
- 33. Each axon innervates 3-10 muscle fibres Precise fine motor control and quick accurate movement of EOMs
- 34. VASCULAR SUPPLY
- 38. MEDIAL MUSCULAR ARTERY LATERAL MUSCULAR ARTERY IR MR IO SR LR SO MR also receives a branch from lacrimal artery IR & IO receives a branch from Infra orbital artery
- 39. FUNCTIONS
- 40. Some Terminologies… AGONIST Any particular EOM producing a specific ocular movement SYNERGISTS Two muscles moving an eye in the same direction ANTAGONISTS Muscles having opposite actions in the same eye
- 41. YOKE MUSCLES ( CONTRALATERAL SYNERGISTS ) A pair of muscles (one from each eye) which contract simultaneously during version movements CONTRALATERAL ANTAGONISTS A pair or muscles (one from each eye) having opposite action
- 42. LAWS GOVERNING OCULAR MOTILITY “ an equal and simultaneous innervation flows from the brain to a pair of muscles of both eyes (yoke muscles) which contract simultaneously in different binocular movements ” HERING’s LAW OF EQUAL INNERVATION
- 44. SHERRINGTON’S LAW OF RECIPROCAL INNERVATION “During ocular motility, an increased flow of innervation to the contracting agonist muscle is accompanied by a decreased flow of innervation to the relaxing antagonist muscle”
- 45. SR IO LR MR IR SO Marquez diagram Right eye
- 47. Remember… All Superior muscles : Intort All Inferior muscles : Extort All Oblique muscles : Abduct
- 49. STRABISM US A misalignment of the visual axes of the two eyes Classification Pseudostrabismus / apparent squint Heterophoria / latent squint Heterotropia / manifest squint
- 51. ISOLATED MUSCLE PARALYSIS most common : paralysis of LR & SO
- 52. LATERAL RECTUS PALSY due to palsy of 6th cranial nerve (abducens) results in convergent strabismus (Esotropia) primary symptom : Diplopia
- 53. SUPERIOR OBLIQUE PALSY palsy of 4th nerve that innervates SO muscles common congenital anomaly associated is Craniosynostosis causes a combination of vertical, horizontal & torsional misalignment of the eyes head tilt / turn is commonly seen to allow better alignment of the eyes; sometimes aiding relief in diplopia
- 55. DOUBLE ELEVATOR PALSY caused by 3rd nerve nuclear lesion characterized by paresis of SR & IO muscle of the involved eye restricted elevation of the eye patient with chin up position to maintain binocularity
- 57. DOUBLE DEPRESSOR PALSY a rare condition paralysis of depressors monocular or unilateral restriction on down gaze
- 59. EXTERNAL OPHTHALMOPLEGIA All EOMs are paralysed Intraocular muscles (sphincter pupillae, ciliary muscle) are spared Due to lesions at the level of motor nuclei ; sparing the Edinger-Westphal nucleus
- 60. TOTAL OPHTHALMOPLEGIA all EOMs including LPS and intraocular muscles becomes paralysed results from combined paralysis of 3rd, 4th & 6th cranial nerves common feature in case of Orbital apex syndrome & Cavernous sinus thrombosis
- 61. DYSTHYROID OPHTHALMOPATHY also k/a Thyroid Eye Disease (TED) / Grave’s Ophthalmopathy characterized by : Proptosis Eyelid retraction Corneal & conjunctival exposure Conjunctival chemosis Chronic TED causes Hypertrophy & fibrosis of EOMs
- 63. REFRENC ES Khurana A. K. , Khurana I. Anatomy & Physiology of Eye Khurana A. K. Comprehensive Ophthalmology Kanski J.J. , Bowling B. Clinical Ophthalmology Previous Presentations Internet….etc
- 65. THANK YOU…..