Rigid internal fixation for mandibular of infected mandibular fractures
•
2 j'aime•1,076 vues


Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (11)
Similaire à Rigid internal fixation for mandibular of infected mandibular fractures
Similaire à Rigid internal fixation for mandibular of infected mandibular fractures (20)
Rigid internal fixation for mandibular of infected mandibular fractures
- 1. J Oral Maxillofac Surg 50:434·443, 1992 Rigid Internal Fixation for the Treatment of Infected Mandibular Fractures MICHAEL KOURY, DDS,* AND EDWARD ELLIS III, DDS, MSt A review of the literature is presented that shows that treatment of infected fractures by rigid internal fixation is biologically sound. A protocol for managing infected mandibular fractures with plate and screw fixation was developed and used on 11 patients. All patients had osseous union of the fracture and none required removal of the bone plate. This protocol is recommended as a viable option in the treatment of infected mandibular fractures. Infected mandibular fractures are common in sur- ternal fixation believe that the best manner to eliminate gical practice because many individuals who sustain the infection is to rigidly immobilize the segments and facial trauma fail to seek immediate treatment. On that, by doing so, bony union will occur irrespective presentation, the patient poses a greater problem when of whether an infection is present. Thus, a dichotomy there is a coexisting infection at the fracture site. Tra- exists in the treatment of such fractures. ditionally, such fractures have been treated with max- When deciding whether to treat a fracture with plate iIIomandibular (MMF) or external fixation. I However, and screw osteosynthesis, the clinician must weigh the with the increasing interest in plate and screw fixation risk of exposing the fracture site and placing a plate in the United States.over the past decade, new methods against the benefits ofabsolute rigidity. In the past two oftreating infected mandibular fractures have been de- decades, research has provided much information veloped. Rigid internal fixation offers many advantages about this dispute. To answer the questions about the to the patient, including no MMF. In spite ofthe grow- viability of the treatment options, a review of the bio- ing interest, most surgeons still.believe that I) metal logical research is necessary. should not be used in contaminated wounds'? and 2) once an infection develops in a internally stabilized Foreign-Body Effect of Implant fracture, the metal must be removed before resolution of the infection can occur. 6-8 However, others believe In orthopedics and oral and maxillofacial surgery, that such materials do not need to be removed from many have emphasized the "foreign-body effect" of a infected sites if rigidity is maintained.v!' Rigid internal metal implant.7 ,10,15 Difficulty exists in accurately de- fixation has even been called the superior treatment termining the biological influence of a foreign body, for infected mandible fractures. 14 because when an implant is placed, surgical trauma is When treating infected mandibular fractures, two inevitably inflicted. If an infection then develops, it is goals exist: 1) resolution of the infection and 2) difficult to determine whether the implant or the sur- achievement of bony union. Those advocating MMF gical trauma and contamination caused the infection. or external fixation believe elimination ofthe infection must occur before bone union occurs. Those using in- Implants Placed Into Clean Wounds The closest approximation ofthe risk assumed solely Received from the Division of Oral and Maxillofacial Surgery, by the addition ofan implant to the body is seen when The University of Texas Southwestern Medical Center, Dallas. placement occurs with minimal soft tissue and vascular • Resident. trauma during a sterile elective procedure. Such is the t Associate Professor. Address correspondence and reprint requests to Dr Ellis: Division case with prosthetic joint replacement. Insall et al re- of Oral and Maxillofacial Surgery, The University of Texas South- ported three deep infections in 220 arthroplasties for western Medical Center, 5323 Harry Hines Blvd, Dallas, TX 75235- total knee replacements." Similarly, Kaufer and Mat- 9031. thews reported three deep infections in 373 total knee © 1992 American Association of Oral and Maxillofacial Surgeons replacements.'? Other orthopedic studies have yielded 0278-2391/92/5005-0002$3.00/0 similar rates of infections when implants are placed 434
- 2. KOURY AND ELLIS 435 into sterile atraumatic wounds.P:'? showing an ex- Varying results have been found in comparative tremely low incidence of infection under these con- studies. Most studies in the orthopedic literature that ditions, in spite of the fact that these implants move have been performed over the past 30 years show that under function. when similar injuries are compared, no major differ- In cases of closed long-bone fractures, the infection ences in the rate of infection are found between those rate is not appreciably greater with internal fixation treated with open reduction with or without internal than with closed reduction. For example, Burri,'? Ole- fixation devices. 3 1•36 Although some studies have shown rod and Karlstrorn." and Allgower" reported infection increased rates of infection for open (contaminated) rates in closed fractures of 0.18% in 744, l.l% in 91, fractures treated with internal fixation when compared and 1.4% in 720 fractures, respectively. Comparable with open reduction without internal fixation, most of rates of infection have also been shown between closed these used internal fixation in wounds where the blood techniques and blind intramedullary nailing. 22,23 supply was greatly disturbed.F:" Soft-tissue injury has been shown to be a primary Implants Placed Into Contaminated Wounds factor in infection rates with internal fixation of con- taminated fractures. Chapman and Mahoney showed A difference in the rate ofinfection between implants a 1.9% infection rate with mild soft-tissue trauma, 8% placed in clean and in contaminated wounds was dem- with moderate trauma, and 41 % in severe soft-tissue onstrated by Rittmann et al. 24 Open and closed tibial trauma of open fractures." Edwards similarly dem- fractures were treated with open reduction and internal onstrated this point and showed the infection rate of fixation with compression plates. He found a 1.8% in- internally fixed fractures could be greatly reduced by fection rate in the closed (noncontaminated) fractures not extending the wound when placing the fixation." and a 6.3% in the open (contaminated) fractures. Like- In dogs, he also found a decrease in the incidence of wise, Burri, in a study of 744 fractures, reported an osteomyelitis when no soft-tissue damage was produced infection rate of 0.18% in closed and 2.7% in open when similar bony fractures were created. These studies fractures treated with internal fixation.'? Towers also may indicate that once contaminated, a fracture treated noted an increased rate of infection in open (contam- with open reduction may be better off with an internal inated) fractures and believed fewer bacteria were fixation device as long as the vasculature and soft-tissue needed to produce clinical infection with metal implant bed is not significantly jeopardized by the additional placement." surgical exposure during implant placement. The body may have difficulty with bacteria in the Overall, the fractured mandible should be very sus- presence ofimplants because biomaterials are a suitable ceptible to infection because of their great tendency to substrata for their growth." Removal of fixation ap- be of the open variety. Mucosal tears and fractures pliances from infected wounds unresponsive to anti- extending through the periodontal ligament produce biotics has revealed bacterial colonization on their sur- contamination of the fracture by the oral flora. 12 Most face. 26 A bacterial biofilm has also been shown on fractures that occur through the tooth-bearing area can orthopedic implants." This surface slime, or glycolax, therefore be regarded as contaminated. Further, sur- is made from carbohydrates of the bacterial cell wall" gical intervention through the poorly cleanable oral and is believed to increase the incidence of infection, cavity further contaminates the wound. Of interest, to provide a barrier to macrophage and antibiotic pen- however, is the finding that a foreign body firmly at- etration, as well as to prohibit the culturability of these tached to bone does not greatly increase the danger of bacteria.P Also, spread of bacteria down nonreactive infection in the mandible.F:" In fact, Luhr et al found biomaterials into noncolonized areas has been fewer infections using an intraoral approach (3.2% in- shown. 29 ,3o In effect, biomaterials alter the body's de- fection) to place fixation devices than when using the fense and provide a surface for bacterial adherence and extraoral approach (5.6%).42 The explanation for these colonization." findings is not clear, but P9ssibly rests with the lush Thus, there is a difference in the rates of infection vascularity in the maxillofacial region. between placing implants in closed (clean) and in open (contaminated) fractures. A comparison must be made, Effect of Mobility on Infection however, between the use of internal fixation devices and not using them when treating contaminated (open) Internal fixation has been called the superior treat- fractures. In other words, when a contaminated fracture ment for infected mandibular fractures," partly be- requires open reduction, does the use of implants alter cause the biological reaction to mechanical influences the rate of infection? Answering this question allows plays an important role in local infection.P Many one to weigh the risk of the foreign body versus the studies have shown that instability promotes infection, benefit of stabilization of the bony fragments and the and stability helps prevent it. 9 , 11. 13, 19,44-46 Friedrich and soft-tissue bed in the presence of bacteria. Klaue showed a correlation between the presence of
- 3. 436 RIGID INTERNAL FIXATION FOR INFECTED MANDIBULAR FRACTURES osteitis and lack of rigidity in rabbit long-bone fractures tion under these circumstances.Y Insall et al 1 and 6 by injecting staphylococcus aureus into rigidly or non- Kaufer and Matthews'? each had three deep infections rigidly fixed sites.'? The group of mobile fractures with 220 and 373 arthroplasties, respectively, that re- without bacterial infection did not become infected, quired implant removal for resolution, but many in showing that even with mobility contamination must orthopedics believe metal implants that provide sta- occur to produce an infection. With mandibular frac- bility should be left in place and only the unstable ones tures, surgeons have made similar suggestions regarding should be removed. I1.19.20 Hicks believed infection was the effect of mobility on the rate of infection. 12,47.48 easy to overcome with rigid internal fixation." Although several authors have stated that implants Effect of Infection on Bone Healing must be removed to resolve infection in the mandible, clinicians have shown resolution without removal as Several authors have shown that bone union can long as the fixation was stable. Johansson et al reported take place in the face of infection both experimentally 42 infected mandibular fractures treated with mini- and clinically.IO·II,13,44,49,so For instance, all of Macaus- plates." Twenty-four percent of the infections persisted land and Eaton's 14 postoperative septic long-bone postoperatively. Six of nine resolved, whereas in the fractures treated with intramedullary rods achieved remaining three the fixation devices were removed be- bony union even though infection was present."? He cause of instability. Beckers showed resolution of all believed complete immobilization promoted osseous 19 infected mandibular fractures he treated with in- union. Similarly, Souyris et al reported 25 cases of ternal fixation." Others also have found resolution of mandibular fracture treated with internal fixation that infection with plates in place when the fractures re- became infected in the early postoperative period." mained stable. 12,52,53,s6-s8 On the other hand, when The plates were left in place for several weeks and, on plates or screws were loose, infections persisted until removal, the bone was found to have healed. Johansson the loose implants were removed. s2,s3,57,59,60 et al,s2 Prein and Schmoker." and Beckers" have shown similar results. Johansson et al found primary Overview bone healing in 76% of cases where infection was present.V The findings from the short review presented led Experimental verification of bone union in the face to the following conclusions regarding placement of of infection was offered by Rittmann and Perren. II fixation devices into contaminated wounds: 1) the risk They conducted osteosynthesis on sheep femurs and ofinfection following open reduction may be no greater infected the stable hone-plated fractures with staphy- than when a device is not placed; 2) bony union can lococci over a period of 8 weeks. All showed bony union occur in the face ofinfection as long as immobilization over this period, some of which" was primary, despite of the fractured segments is maintained; 3) resolution the clinical infections. The study by Friedrich and of infection can occur even when a plate is present; 4) KIaue of rabbit long-bone fractures stabilized internally if resolution of an infection does not occur in a fracture and infected with Staphylococcus aureus also showed treated with internal fixation, one must verify that the that primary bone union occurred in the face ofinfec- fixation is rigid; 5) if resolution of an infection does tion as long as the osteosynthesis was stable.':' not occur in a fracture treated with stable internal fix- Conversely, mobility of an infected fracture is not ation, one can usually leave the plate for 8 to 12 weeks well tolerated. Meyer et al treated 214 cases of osteo- to achieve bone union, and then remove it to allow myelitis after operative treatment of fractures; 45 of rapid resolution of the infection. 49 fractures that had unstable fixation resulted in non- Given these findings, we developed a simple protocol union." Furthermore, in the presence of infection, for treating infected fractures with internal fixation in- nonsurgical treatment may not be effective because of tending not to remove the plates. Choice of treatment the lack of rigidity, as demonstrated by Nicol1.54 He is predicated on the extent of the infection. If a patient treated 22 infected long-bone fractures nonsurgically, presents with a mild to moderate cellulitis or a spon- with a resulting 60% incidence of delayed union or taneously draining abscess, the patient is treated by nonunion. open reduction and internal fixation, with placement of a drain for postsurgical irrigation with saline. Intra- Infection Following Osteosynthesis venous antibiotics are given in the perioperative period. If a patient presents with a severe cellulitis or closed Once an infection develops in a fracture stabilized (nondraining) abscess, the patient is treated as any pa- with internal fixation, can one obtain complete reso- tient with an infection, with intravenous antibiotics lution of the infection with the implant in place? Many and incision and drainage in the case of an abscess. clinicians in orthopedics and maxillofacial surgery have After 3 to 4 days, the patient is taken to surgery for stated that implants must be removed to resolve infec- open reduction and internal fixation of the fracture. A
- 4. KOURY AND ELLIS 437 drain is left following surgery for continued saline ir- bacterium. Two days later, with gross purulence absent, the rigation. In either of the preceding courses oftreatment, drain was removed and the patient was taken to the operating room and given cefazolin (I g every 6 hours). Under general any other potential cause for the infection, such as a anaesthesia, an intraoral incision was made and granulation devitalized tooth, is eliminated as soon as possible. tissue was removed from the fracture site. Arch bars were We have used this protocol for the past 2 years and placed, MMF secured, and a bone clamp was used to reduce have found it to be effective. Frequently, owing to the fracture. A six-hole reconstruction plate was placed in- scheduling difficulties, the timing of surgical interven- traorally in a noncornpressive manner along with a Penrose tion may be expedited or delayed, but we generally drain; the MMF was then released (Fig IB). Four days later, the antibiotic was changed to ticarcillin/clavulonate (3.1 g attempt to institute the protocol described. Two cases every 6 hours). Slight purulence was noted at this time, but representative ofour experience with placement of rigid stable fracture segments and occlusion were present. The fol- internal fixation in infected mandibular fractures are lowing day, an intraoral communication was noted but the presented. Nine additional cases are presented in Table wound was free of purulence and granulation tissue was I. Contrary to previously reported cases, the fixation forming at the wound site. After drain removal the following day, the patient was given amoxicillin/clavulonate (500 mg devices were not removed. every 8 hrs) and discharged. Ten days later the patient re- turned to the clinic without complaint. At this time he had a good range of motion, normal sensation in his lower lip, Report of Cases and resolution of the swelling. The arch bars were removed that day. The patient was seen 26 weeks following fracture Case 1 and was found to be doing well. His occlusion was normal (Fig IC), and the fracture had healed completely with no A 31-year-old woman was struck in the face several days signs of residual infection (Fig ID). prior to seeking care. The patient had poor oral hygiene, malocclusion (Fig IA), submental space abscess (Fig IB), mobility between the first premolar and canine, and an in- Additional Cases terincisal opening of 30 mm. Radiographic evaluation re- vealed a minimally displaced left body fracture and a mod- Nine additional cases are presented in Table l. All erately displaced right subcondylar fracture (Fig IC). The of these cases were treated by 2.7-mm bone plating patient was admitted to the hospital and treated with intra- systems. Follow-up in all cases showed resolution of venous penicillin G (2 million units four times hourly). Two infection, stability across the fracture to bimanual pal- days later, she was taken to the operating room, where an incision and drainage of the' submental abscess was per- pation, good occlusal relationships, and no clinical or formed, followed by application ofarch bars and MMF. The radiographic signs of nonunion. fracture in the mandibular body was opened transorally and rigidlysecured with the placement ofa six-hole reconstruction Discussion plate at the inferior border of the mandible after the removal ofa small sequestrum (Fig ID). A Penrose drain was placed through the extraoral incision and drainage incision into the The cases presented support the findings of other subperiosteal space (Fig IE). No postsurgical MMF was used. authors in orthopedics9,I1,2o,46,49 and oral/maxillofacial Two days later, with the patient progressing well and with surgeryl2,14,52,58 where internal fixation has been used no purulent drainage, the drain was removed and she was to treat infected fractures. The majority ofthese authors discharged with a prescription for cephalexin (500 mg four removed the fixation appliance after bony union oc- times daily). At this time, the patient had moderate swelling around the chin. By the following week the swelling had re- curred. We have found that fracture union and reso- solved. Eight weeks later, the patient had an interincisal lution of infection can be accomplished without re- opening of45 mm and was without complaint. The arch bars moval of the plate. Using our experience in the were subsequently removed and 55 weeks after injury she treatment of infected fractures with rigid internal fix- was doing well without further complications (Figs IF,IG). ation and those fractures that had become infected fol- lowing application of rigid internal fixation, we devel- Case 2 oped a protocol for treating infected mandibular A 32-year-old man sustained a fracture of the mandibular fractures. symphysis 3 weeks prior to coming to the emergency de- As with any patient, a careful history and physical partment. He complained of swelling and draining pus. lie examination are performed. After the diagnosis is was afebrile, had submental swelling with extensive overlying made, the patient is given antibiotics, preferably intra- erythema, and had a sinus tract in the submental area that occasionally drained spontaneously. Intraorally, the mucosa venous, and is usually admitted to the hospital. A de- was open, with exposed bone. An occlusal step was apparent cision must then be made whether to treat the infection on the left side, and the left lower lip was anesthetic. A di- before reduction and internal fixation of the fracture. agnosis of open, infected, minimally displaced mandibular This decision is predicated largely on the basis of the symphysis fracture was made (Fig 2A). The patient was ad- vascularity of the region and severity of the infection. mitted to the hospital, treated with intravenous penicillin G (2 million units every 4 hours) and a submental incision and The vascularity of the tissue has been found to be ex- drainage was done. Initial cultures revealed coagulase-positive tremely important for preventing and overcoming an staphylococcus, clostridium, peptostreptococcus, and fuso- infection, especially in the presence of an avascular
- 5. ~ (j.) ex> Table 1. Cases of Infected Mandibular Fractures Treated With Rigid Internal Fixation Age Infected Duration of Previous Treatment Rendered for Patient Sex (yr) Fracture Infection Treatment Type of Infection Infected Mandibular Fracture Follow-up (wk) 3 F 29 Symphysis 1 wk Oral PCN X I wk Nondraining abscess IV PCN, simultaneous I/O I & 17 prior to with overlying D and ORIF with four-hole presentation cellulitis in compression bone plate, E/ ;;0 submental space o drain; drain removed 2 d s postop; DC 2 d postop; at 7 S d, readmission with submental infection; IV ~ m ;;0 amoxieillin, E/O I & D, E/O z drain placed;drain removed > ["" 2 d postop; DC 3 d postop 74 :!l 4 M 3 Rt angle >1 mo Closed reduction Spontaneously draining 6 d of IV PCN; simultaneous X of same (I/O) submandibular E/O I & Dand > -l fracture 5 mo space abscess, debridement, ORIF with 0 before; no sequestra formation eight-hole noncornpression Z follow-up reconstructive bone plate, .,., 0 extr no. 31, E/O drains; ~ drains removed 5 d postop; Z DC6 d postop ril 5 M 27 Lt angle 3 wk Oral PCN X I wk Spontaneously draining IV ccphazolin, E/O I & D and 21 ::J tn prior to (I/O) subperiosteal ORIF with noncompression C presentation abscess at eight-hole reconstructive mandibular angle bone plate + four-hole 2- z > . mm plate at superior Z C border, E/O drains; drains tii removed I d postop; DC 2 e d postop !;: ;;0 6 M 33 Symphysis 2wk None Localized cellulitis and IV PCN,I/O I & D and ORIF 15 swelling with erythema of with seven-hole noneompression ~ submental skin reconstructivebone plate, ::J c no drain placed; DC same ~ day I3l
- 6. 7 M 28 Lt body 3d ORI F with lag Localized alveolar IV PCN, I/O I & D, hard ware 20 ~ swelling, 0 screw and 2· removal (hardware was c: mm bone plate spontaneous- loose), sequestrectomy, and :;0 of fractur e 5 draining (I/O ) ORIF with six-hole -< wk earli er submandibular space noncompression > Z ab scess, non un ion of reconstructive bone plate, 1/ 0 tTl fx o drain; drain removed 2 d r- r- postop; DC 4 d postop Vi 8 M 33 Rt body 2 wk Non e Spontaneous-drainin g IV PCN, E/O I & D and ORI F 13 (I/O ) submandibular with eight-hole space abscess noncom pression reconstructive bone plate, E/O drains; drain remo ved 2 d postop; DC 3 d postop 9 F 34 Rt bod y 5 wk Closed reduction Spontaneous-draining IV PeN, E/O I & D and 14 of fracture 6 (I/O ) subm and ibula r sequestrectomy. ORIF with wk earlier space abscess, seven-hole noncomprcssion sequestra formation reconstructive bone plate. E/O drains; drain removed 2 d postop; DC 3 d postop 10 M 32 Rt angle 3 wk ORI Fof same Spon taneous-drainin g IV PCN, E/O I & D and 31 fracture 5 wk (I/O) subm andi bular seq uestrectomy, ORIF with prior with two space abscess, eight-hole noncom pression 2-mm plates sequest ra format ion reconstructive bone plate, E/O drains; drain removed 3 d postop ; DC 4 d postop II M 28 Lt a ngle 1 wk None Submandibular/ IV PeN. E/O I & D a nd ORI F 16 subperiosteal abscess with eight-hole lateral mand ible. noncom pression fluctuant reconstructive bone plate. E/O drains; drains remo ved 2 d postop; DC 3 d postop All bone plates were appli ed with 2.7-mm bone screws. Abbreviations: E/O . extraoral ; I/O , intraoral; I & D. incision a nd drainage; PCN, penicillin G ; ORIF, open reduction and internal fixat ion; DC, discharge. .j:Io. c.:l <0
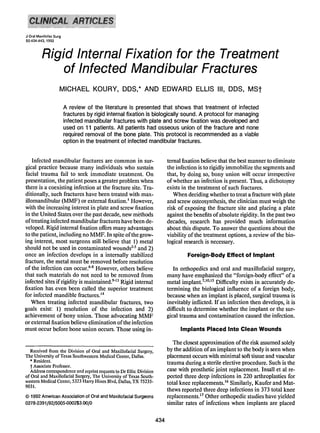
- 7. 440 RIGID INTERNAL FIXATION FOR INFECTED MANDIBULAR FRACTURES B FIGURE I. Patient with infected mandibular symphysis fracture. A. Malocclusion. B. Submental abscess. C, Panoramic radiograph of patient showing symphyseal fracture and right subcondylar fracture. E, Six-hole reconstruction bone plate used to stabilize the fracture. Note small piece of bony sequestrum in forceps (below). D, Immediately postsurgery, showing Penrose drain in place. F. Occlusal relationship at 55 weeks postsurgery. G, Panoramic radiograph at 55 weeks postsurgery.
- 8. KOURY AND ELLIS 441 AGURE 2. Patient with infected mandibular symphysis fracture. A. Panoramic radiograph showing fracture. B. Intraoperative photograph showingfracture reduced with a reconstruction bone plate. C. Occlusionat 26 weekspostsurgery. D, Panoramic radiograph 26 weekspostsurgery. implant. 33,38,4o,61,62 If there is only a mild to moderate step necessitates the removal of teeth in the line of the cellulitis or a spontaneously draining abscess, we per- fracture that are indicated for extraction,52,53.63 curet- form the open reduction and internal fixation as soon tage of granulation and infected soft tissue, sauceri- as our operating room schedule permits. Drains are zation and sequestrectomy of dead bone, and the re- placed if gross purulence is noted intraoperatively. If moval of nonfunctional foreign bodies. 7.9,44,46,64 severe cellulitis is present, intravenous antibiotics are Second, if drains are deemed necessary due to the pres- given until the tissue pressure has decreased to allow ence of purulence in the wound at the time of surgery, improved perfusion of the area for better healing and they must be kept in place until the wound stops pro- resolution of the infection. Likewise, if copious purul- ducing such drainage. 46,52 The drains allow the wound ence has caused extensive tissue dissection and abscess to be irrigated and also prevent the build-up ofabscess loculations, implant placement may be best accom- cavities that the body is unable to fight efficiently. One plished a few days after incision and drainage to relieve should not be too quick to remove the drains in such the tissue tension. Any devitalized teeth are removed patients. Third, absolute rigidity is essential. Rigidity as early as possible. In such cases, the drains are irri- has been shown to produce a stable foundation for soft- gated four times daily. Once the swelling and purulence tissue growth " so that vascularity to the area can im- have decreased, the patient is taken back to the oper- prove and the wound can heal." Avascularity has been ating room for open reduction and rigid fixation. Sim- shown to be one of the primary risk factors for infec- ilarly, infected wounds with a large area of necrotic tion. 37,39 Rigidity has also been shown to prevent bac- and avascular tissue and comminuted fragments, such teria from being continually pumped through the frac- as infected gunshot wounds, may be better treated ture site, thereby decreasing the chance of osteitis.'? without extensive surgical intervention until the infec- One must remember that osteolysis occurs in the pres- tion begins to resolve and viability of the soft tissues ence of infection, which can weaken the bone sur- is established. Typically, when surgery is delayed, it is rounding the screws. I 1,13 This increases the possibility usually performed approximately 3 to 4 days following of fragment mobility and delayed bone healing. Be- incision and drainage. cause of these considerations, greater rigidity is nec- When using rigid internal fixation devices for in- essary. We most commonly employ heavy reconstruc- fected mandibular fractures, three points should be tion bone plates with 2.7-mm bone screws to secure borne in mind. First, adequate debridement of infected such fractures. In the mandibular angle region, and tissue is essential for resolution of the infection. to This usually elsewhere in the mandible, three screws are
- 9. 442 RIGID INTERNAL FIXATION FOR INFECTED MANDIBULAR FRACTURES placed on each side of the fracture to assure firm fix- This treatment is not proposed as a replacement for ation. When the bone fragments have not been eroded more traditional methods. Both external fixation and by the infective process, we may employ the use of MMF have stood the test of time and proved their compression osteosynthesis. Compressing the bone effectiveness. Rather, plate and screw fixation is a viable fragments provides more rigidity for a given number option that allows the patient the same benefits that of bone screws." Compression also helps reduce the its use in noninfected fractures provides. It is very useful fracture gap,65 thus decreasing the chance of osteitis in the noncompliant patient who frequently will not and the progression of the infection.I':'? In 1979, tolerate MMF. Beckers" reported 14 infected fractures in which four of five treated without compression developed post- References operative infections, whereas only one of nine with compression became infected. Reduction of the bone I. Topazian RG, Goldberg MH: Oral and Maxillofacial Infections. gap and absolute rigidity also promoted primary bone Philadelphia, PA, Saunders, 1977 pp 216-218 2. Soto-lIiII R, Horwitz T: The treatment of compound fracture union;,,1J·52 expediting the healing time.'? of the femur. JAMA 130:128, 1946 During the course of healing, resolution of the in- 3. Watson-Jones SR: Primary internal fixation of compound frac- fection and stability of the fracture must be assessed. tures. J Bone Joint Surg IBr] 35:147, 1953 4. Towers AG: Wound infection in an orthopaedic hospital. Lancet Usually both will proceed uneventfully.lv'? but if pu- 2:380,1965 rulent drainage continues after drain removal, surgical 5. Ketenjan AY, Shelton ML: Primary internal fixation of open treatment is indicated. The usual causes of persistent fractures: a retrospective study of the use of metallic internal fixation in fresh open wounds. J Trauma 12:756, 1972 drainage are I) an odontogenic infection;5,47.52.62 2) 6. Dahl-Iverson E: On the frequency and the duration of osteitis sequestra, or 3) loose fixation. 52,53,63 Treatment of the after osteosynthesis illustratedby 274 casesand re-examination latter two usually cannot be accomplished under local of 66 cases of operatively treated fractures. Acta Chir Scand 63:41, 1928 anesthesia. Iflarge sequestra are seen radiographically, 7. Reynolds FC, Zaepfel F: Management of chronic osteomyelitis or if the fracture is mobile, the patient will most likely secondary to compound fractures. J Bone Joint Surg [Am] need to be taken back to the operating room for de- 30:331, 1948 8. Gustilo RB, Simpson L, Nixon R, et al: Analysis of 511 open bridement in the former case and restabilization in the fractures. C1in Orthop 6:148, 1969 latter. '9,52 Correction of these conditions normally re- 9. KeyJA, ReynoldsFC: The treatment of infectionafter medullary sults in resolution of the infection, but occasionally nailing. Surgery 35:749, 1954 10. Rowe CR, Sakellarides lIT: Recent advances in the treatment minor purulence will remain. If drainage is still oc- of osteomyelitis following fracture of the long bones. Surg curring after a period in which union is likely, the plate C1in North Am 41:1593, 1961 can be removed." Usually, as long as the fixation has I I. Rittmann WW, Perren SM: Cortical Bone HealingAfter Internal Fixation and Infection. New York, NY, SpringerVerlag. 1974 remained stable, union will occur even if an infection 12. SchilliW: Compression osteosynthesis.J Oral Surg 35:802, 1977 was present. II,13,14,51 Often, it is found that loose fixa- 13. Friedrich B, Klaue P: Mechanical stability and post-traumatic tion propagated the infection. 51,53,57,59 Resolution of osteitis: An experimental evaluation of the relation between infection of bone and internal fixation. Injury 9:23, 1977 the infection usually proceeds rapidly after the non- 14. Beckers HL: Treatment of initially infected mandible fractures functional foreign body is removed.f with bone plates. J Oral Surg 37:310, 1979 If during the course of healing the implant becomes 15. StrelzowVV, StrclzowAG: Osteosynthesis of mandible fractures in the angle region. Arch Otolaryngol 109:403, 1983 exposed, the treatment decision is again predicated on 16. Insall J, Scott WN, Ranawat CS: The total condylar knee pros- whether the fracture is mobile. 58.6o If the fracture is thesis. J Bone Joint Surg [Am] 61:173, 1979 stable, the bone is allowed to achieve union and then 17. Kaufer H, Matthews LS:Spherocentric arthroplasty of the knee. J Bone Joint Surg [Am] 63:545, 1981 the plate is removed." Removal is frequently necessary 18. Sheehan JM: Arthroplasty of the knee. J Bone Joint Surg [Br] because soft tissue does not always cover an exposed 60:333, 1978 plate." 19. Burri C: Post-TraumaticOsteomyelitis. Bern, Hans Huber, 1975, pp 19-125 20. OIerud S, Karlstrorn G: Tibial fractures treated by AO compres- Conclusion sion osteosynthesis. Acta Orthop Scand 140:1, 1972 (suppl) 2 I. AllgowerM: Weichteilprobleme und infektionsrisike dcr osteo- Our experience and that of others in both orthope- synthese, Langenbecks Arch Klin Chir 329:1127, 1971 dics and oral/maxillofacial surgery indicates the use of 22. Lottes JO, llill U, Key JA: Closed reduction, plate fixation and internal fixation is a plausible treatment for infected medullary nailing of fractures of both bones of the leg.J Bone Joint Surg [Am] 34:861, 1952 mandible fractures. The following reasons are note- 23. D'Aubigne RM, Maurer P, Zucman J, et al; Blind intramedullary worthy: l) fracture union and resolution of infection nailing for tibial fractures. Clin Orthop 105:267, 1974 are predictably achievable; 2) if, after using rigid fixa- 24. Rittmann WW, Schibli M, Matter P, ct al: Open fractures: long- term results of 200 consecutive cases. Clin Orthop 138:132, tion the infection is prolonged, bone union can still 1979 occur; 3) if resolution of infection is delayed, the im- 25. Gristina AG, Costerton JW, Leake E, et al: Bacterial colonization plant can be kept in place until after bone union; un- of biornatcrials. C1inLab Stud Orthop Trans 4:355, 1980 26. Nishioka GJ, Jones JK, Triplett RG, et al: The role of bacteria- eventful wound healing will then occur following im- laden biolilmsin infection of maxillofacial biomaterials, J Oral plant removal. MaxillofacSurg46:19,1988
- 10. BUCHDINDER AND WEBER 443 27. Costerton JW, Geesey GG, Cheng KJ: 1I0w bacteria stick. Sci non-union of fractures of long bones. J Bone Joint Surg 57: Am 238:86,1978 836, 1975 28. Gristina AG, Kolkin J: Current concepts review-Total joint 47. Kellman RM: Repair of mandibular fractures via compression replacementand sepsis. J BoneJoint Surg [Am] 65:128, 1983 plating and more traditional techniques: A comparison of re- 29. Gristina AG, Rovere GO: An in vitro study of the effects of sults, Laryngoscope 94:1560, 1984 metals used in internal fixation on bacterial growth and dis- 48. KlotchOW, Bilger JR: Platefixation for open mandiblefractures. semination. J Bone Joint Surg [Am] 45:1104, 1963 Laryngoscope 95:1374, 1985 30. Gristina AG, Revere GO, Shoji II, et al: An in vitro study of 49. Macausland WR, Eaton RG:The managementofsepsis following bacterial response to inert and reactive metals and to methyl intramedullary fixation for fracture of the femur. J BoneJoint methacrylate. J Biomed Mater Res 10:273, 1976 Surg [Am] 45:1643, 1979 31. Holstad HA: Primary osteosynthesis versus conservative treat- 50. Carr CR, Turnipseed CD: Experience with intramedullary fix- ment of compound fractures of long tubular bones. J Oslo ation of compound femoral fractures in war wounds.J Bone City Hosp 12:225, 1962 Joint Surg [Am] 35:153.1953 32. Wade PA, Campbell RD: Open versusclosed methodsin treating 51. SouyrisF, LamarcheJP, Mirfakhrai AM:Treatment of mandible fractures of the leg. Am J Surg 95:599, 1958 fractures by intraoral placement of bone plates. J Oral Surg 33. Solheim K: Fractures of the lowerleg.Acta Chir Scand 119:268, 38:33, 1980 1960 52. Johansson B, Krekmanov L, Thomasson M: Miniplate osteo- 34. Bauer GC, Edwards P, Windmark PII: Shaft fractures of the synthesis of infected mandibularfractures. J Cranio Maxillofac tibia: Etiologyof poor results in a consecutive series of 173 Surg 16:22, 1988 fractures. Acta Chir Scand 124:386, 1962 53. Prein J, Schmoker R: Treatment of infected fracturesand pseu- 35. Edwards P: Fracture of the shaft of the tibia: 492 consecutive doarthrosis of the mandible, III Spicssl B (ed): New Concepts cases in adults. Acta Orthop Scand 76:I, 1965 (suppl) in Maxillofacial BoneSurgery. NewYork, NY,Springer, 1976, 36. Wehner W: Wandlung in der behandlung komplizierter langer pp 169-174 sehaftknocjenfrakturen. Z Artz FortbiId 62:1313, 1968 54. Nicoll EA: Fracture of the tibial shaft. J Bone Joint Surg [Br] 37. GustiIo RB, Anderson JT: Prevention of infection in the treat- 46:373, 1964 ment of 1025open fracturesof long bones. J BoneJoint Surg 55. Hicks HI: Amputations in fractures of the tibia. J Bone Joint [Am] 58:453, 1976 Surg [Br] 46:388, 1964 38. Gallinaro P, Grova M, Dcnicolai F: Complications in 64 open 56. Frost DE, EI·Atlar A, Moos KF: Evaluation of metacarpal bone fracturesof the tibia. Injury 5:157, 1974 plates in the mandible fracture. Br J Oral Surg 21:214, 1983 39. Chapman MW, Mahoney M: The role of early internal fixation 57. Tu 11K, Tenhulzen D: Compression osteosynthesis of mandible in the management of open fractures. Clin Orthop 138:120, fractures: A retrospective study. J Oral Maxillofae Surg 43: 1979 585, 1985 40. Edwards P: The effect of crush injury to the skin on healing of 58. Prcin J, Beyer M: Management of infection and nonunion in fracturesof the shaft of the tibia in dogs. Acta Orthop Scand mandibular fractures. Oral Maxillofac Surg Clin North Am 36:89, 1965 2:187, 1990 41. Niederdellrnann II, Akuarnon-Boatcng E: Internal fixation of 59. Cawood J1: Small plate osteosynthesis of mandibular fractures. fractures. Int J Oral Surg 7:252, 1978 Br J Oral Maxillofac Surg 23:77, 1985 42. Luhr IIG: Comparative studies between the extraoral and in- 60. Assael LA: Complications of rigid internal fixation of the facial traoralapproach in compression-osteosynthesisof mandibular skeleton. Oral Maxillofae Surg Clin North Am 2:615, 1990 fractures, ill Hjorting-Hansen E (cd): Oral and Maxillofacial 61. Hicks JH: High rigidity in fractures of the tibia. Injury 3:121, Surgery. Proc 8th Inti Conf Oral Maxillofac Surg. Chicago, 1971 IL, Quintessence 1985, pp 133-137 , . 62. StrelzowVV, Friedman W: Dynamiccompression platingin the 43. Muller ME, Allgowcr M, Schneider R, et al: Manual oflnternal treatment of mandibular fractures. Arch Otolaryngol 108 :583, Fixation (ed 2). Berlin, Springer-Verlag, 1979, pp 152,306 1982 44. Brav EA, Jeffress VH: Intramedullary nailing in recent gunshot 63. Buchbinder D: Use of rigid internal fixation in the treatment of fractures of the femoral shaft. J Bone Joint Surg [Am] 35: mandible fractures. Oral MaxillofacSurg Clin North Am 2: 141,1953 41,1990 45. Rush ilL, Fills VT, Gibbons J, et al: Intramedullary nailing in 64. Dramula JO, AjagbcHA: Chronic osteomyelitisof the mandible the presenceof infection. Surg Gynecol Obstet 94:727, 1952 in adults: A clinical study of 34 cases. Br J Oral Surg 20:58, 46. MeyerS, Weiland AJ, Willenegger H: The treatment of infected 1981 J Oral Maxillofac Surg 50:443-444. 1992 Discussion Rigid Internal Fixation for the Treatment fixation applied according to established biomechanical of Infected Mandibular Fractures principles have been well documented.' Early, pain-free mo- bilization of the mandible without jeopardizing healing has come to include application of these techniques in recon- Daniel Buchbinder, D/lfD, and structivc and orthognathic procedures as well as in the treat- William Weber, DMD ment of infected fractures'" and delayed treatmcnr'" of non- The Mount Sinai School ofMedicine and Medical Center, infected fractures. Reports of early immobilization as a Nell' York prerequisite for considering RIF have been unconvincing.t Cases for rigid internal fixation, like any other treatment; The authors' presentation of II cases of open reduction must be carefully selected. As the authors suggest, it should and rigid inlernal fixation (RIF) of infected mandibular frac- be strongly considered in the treatment of noncompliant pa- tures using their treatment protocol further shows the use- tients who will not tolerate MMF. Although many cases of fulness and, when properly performed, efficacy of RIF in infected fractures may involve a noncompliant patient pop- maxillofacial traumatology. The benefits of absolute rigid ulation, some infected cases are the result oftreatment delayed