Islet cell Pathology
•
7 j'aime•3,100 vues

Islet cell Pathology and suggestive Slides, insulin activity,comparison

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Islet cell Pathology
Similaire à Islet cell Pathology (20)
Dernier
Dernier (20)
Islet cell Pathology
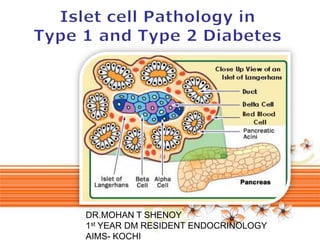
- 1. DR.MOHAN T SHENOY 1st YEAR DM RESIDENT ENDOCRINOLOGY AIMS- KOCHI Page 1
- 2. 1869 German anatomy student Paul Langerhans first described “islands of clear cells ” distributed throughout the pancreas but he did not realize the physiologic significance of these cell clusters, which are today known as islets of Langerhans. We now know that islets are the endocrine compartment of the pancreas, comprising around 2 – 3% of the total pancreatic volume. Islets are approximately spherical with an average diameter of 100 – 200 μ m, and a healthy human pancreas may contain up to a million individual islets, each having its own complex anatomy, blood supply and innervation.
- 3. Page 3
- 4. Page 4
- 5. 98% of organ produces digestive enzymes (exocrine) Composed of acini and ducts Acini cuboidal to columnar cells with cytoplasmic zymogen granules Ducts are lined by columnar epithelium Fat, alcohol stimulate secretin, cholecystokinin production These stimulate 2-2.5 liters of alkaline enzyme containing fluid per day
- 6. Functional definition (Dr. McDonald): “a group of diseases characterized by high levels of blood glucose resulting from defects in insulin secretion, insulin action, or both.” Pathologic Anatomy: Chronic hyperglycemia leads to: 1) accelerated atherosclerosis in arteries 2) altered basement membranes in small vessels RESULT: damage to multiple organs
- 8. LONG-TERM PATHOLOGIC EFFECTS ARE THE SAME IN BOTH TYPES These effects are extremely variable and quite unpredictable for any given patient regarding: SEVERITY DISTRIBUTION RATE OF APPEARANCE OVER TIME Organs affected in addition to pancreas: Macrovascular disease: accelerated atherosclerosis causes ischemia of heart, kidneys, brain, lower extremities Microvascular disease: kidneys, eyes, nerves
- 11. Primary abnormality: failure of self-tolerance in T cells Autoreactive T cells survive ( ? defective clonal deletion in thymus or failure of regulatory T cells) T cell activation in peripancreatic lymph nodes and pancreas, recognizing antigens released from damaged cells Secondary events: development of antibodies Anti-islet cell Anti-glutamic acid decarboxylase 65 (GAD 65)
- 12. There are nearly 1 million islets of Langerhans in the normal adult pancreas. They vary greatly in size from 40 to 900 μm. Larger islets are located closer to the major arterioles and smaller islets are embedded more deeply in the parenchyma of the pancreas. Most islets contain 3000 to 4000 cells - Islets are highly vascularized, and receive up to 15% of the pancreatic blood supply despite accounting for only 2 – 3% of the total pancreatic mass. Each islet is served by an arteriolar blood supply that penetrates the mantle to form a capillary bed in the islet core. β - cells comprise 60 – 80% of the islet cell population Islets are well supplied by autonomic nerve fibers and terminals containing the classic neurotransmitters acetylcholine and norepinephrine, along with a variety of biologically active neuropeptides.
- 13. 1 million 100-200 mm islets total 1-1.5g 5 major types β cells 70% of cells (Insulin) α cells 20% of cells (Glucagon) δ cells (Somatostatin) Є cells that secrete Ghrelin, and PP cells that secrete Pancreatic Polypeptide 2 minor cell types: D1 (VIP) & Enterochromaffin cells (serotonin) MALLORY-AZAN STAIN α cells – Brilliant Red β cells – Orange Brown δ cells - Blue
- 14. 1-2% of body wt (in adults) 5% of body wt (in infants) Combined wt of all islets = 1-1.58 gm β cells - More on dorsum and in tail region adj. to spleen
- 15. In humans, β cells generally located in central part, mostly hererochromatic nature. Islet cells > 0.4 mm diameter = hypertrophic Largest cells are centrally located with pink cytoplasm, larger nuclei, prominent nucleoli and coarse chromatin. Islet cells are not static – apoptosis occurs to remove cells - multiplication by cell division and nesidioblastosis
- 20. “PEACOCK with PLUMES spread out” – curvilinear arrangement of glomeruloid islets with hilum and vascular pattern
- 24. Lesions not pathognomonic, generally more severe in type I than type 2 Both types: Decreased numbers of islets Increased islet size and number in infants of mothers with overt or gestational DM Type I: T-lymphocytic infiltrate/insulitis Progressive depletion of cells -Later small indistinct or absent islets Fibrosis of islets Type II: Amyloidosis of islets Ill defined reduction in islet cell mass Fibrous tissue accumulation in some islets
- 25. Islet of Langerhans (black oval) with surviving islet cells (inside blue shapes) after islet cell destruction by many infiltrating lymphocytes Fig. 24-33 A, Robbins Pathologic Basis of Disease, 8th ed, Elsevier 2010
- 26. ISLET AMYLOID A pathologic feature present in 90% of patients with T2DM is the abnormal extracellular deposits of islet amyloid. These deposits are localized in the pancreas and are not part of a systemic amyloidosis disorder. The islet amyloid is formed from IAPP or amylin, a 37 amino acid peptide. IAPP is normally produced by the β - cell, stored along with insulin in its secretory granules, and then co secreted with insulin following β - cell stimulation. IAPP has no known physiologic function in human
- 29. Most common islet cell tumor 5-10% metastasize Presents with hypoglycemia (<50mg/dl), confusion/stupor with fasting/exercise, symptoms improve with food
- 30. Gritty gray hard masses ; Vast majority are adenocarcinomas, with poorly formed glands and densely fibrous stroma Carcinoma of pancreatic head: invasion of ampullary region with bile outflow obstruction, & distension of biliary tree
Notes de l'éditeur
- Retroperitoneal, inferior and dorsal to stomach
- Insulin (from cells)secreted after meal with carbohydrates raises glucose blood levelsstimulates glucose and amino acid uptakenutrient storage effect (stimulates glycogen, fat and protein synthesisantagonizes glucagon