Chylothorax
•Télécharger en tant que PPTX, PDF•
46 j'aime•11,443 vues

etiology , diagnosis , treatment

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Chylothorax
Similaire à Chylothorax (20)
Plus de Vijay Anand
Plus de Vijay Anand (14)
Dernier
Dernier (20)
Chylothorax
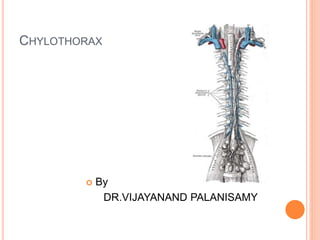
- 2. Thoracic duct - Is the largest lymphatic trunk which drains chyle(product of fat digestion) & most lymph of body. - Extent- Upper abdomen at lower border of T12 to lower part of neck, crossing post & sup mediastinum - 45cms long & 0.5cms wide - Appears Beaded due to presence of many valves in its lumen 2
- 3. Drains lymph from whole of body except • Rt side of head & neck • Rt upper limb • Rt lung & thoracic wall • Rt side of heart and rt surface of liver AREA OF DRAINAGE 3
- 5. COURSE: * BEGINS IN ABDOMEN AT LOWER BORDER OF T12 AS A CONTINUATION OF CISTERNA CHYLI * ENTERS POST MEDIASTINUM THROUGH AORTIC OPENING OF DIAPHRAGM(T12) * AT T5 SHIFTS TO LEFT & RUNS IN SUPERIOR MEDIASTINUM * AT C7 (ROOT OF NECK) ARCHES LATERALLY, THEN DOWNWARDS * ENDS AT ANGLE FORMED BY UNION OF LEFT INT JUGULAR VEIN & LT SUBCLAVIAN VEIN, (REGURGE OF BLOOD PREVENTED BY A PAIR OF VALVES)
- 6. COMPOSITION OF CHYLE Lipids - 60% to 70% of ingested fat absorbed by intestinal lymphatics. Proteins Electrolytes Cellular Elements Miscellaneous Elements - Fat soluble vitamins, antibodies, urea nitrogen, and enzymes
- 7. CHYLOTHORAX A chylothorax (or chyle leak) is a type of pleural effusion. It results from lymph formed in the digestive system called chyle accumulating in the pleural cavity due to either disruption or obstruction of the thoracic duct. In a normal adult, the thoracic duct transports up to 4 L of chyle per day, allowing a rapid and large accumulation of fluid in the chest The prevalence after various cardiothoracic surgeries is 0.2-1%.
- 8. CHYLOMA a collection of chyle below the pleura develops when the thoracic duct first leaks severe chest pain, dyspnoea and tachycardia
- 9. AETIOLOGY
- 10. subclavian vein catheterisation and duct blockage due to central venous catheterisation related venous thrombosis Yellow nail syndrome-bronchiectasis, sinusitis , hypoplastic lymphatics, yellow nails (due to slow growth), lymphoedema, particularly of the lower limbs and pleural effusions
- 11. SIGNS AND SYMPTOMS Hypovolaemia Respiratory difficulty malnutrition due to the loss of protein, fats and vitamins - weight loss and muscle wasting hyponatraemia and hypocalcaemia Immunosuppression Empyema is a rare due to bacteriostatic nature of lecithin and fatty acids Decreased breath sounds Shifting dullness
- 12. Congenital Chylothorax-Fluid initially clear but turns turbid with milk feeding
- 13. The effusion may be unilateral, either right (50%) or left sided (33.3%), or bilateral (16.66%) and is dependent on the location of the leak. Damage to the duct above the fifth thoracic vertebra results in a left sided effusion whereas damage to the duct below this level leads to a right sided effusion
- 14. INVESTIGATION confirmation of the diagnosis by fluid analysis identification of the leakage point Investigation should continue until the aetiology
- 15. fluid will not always be milky or white and may for example be blood stained after trauma or even serious in appearance if the patient is fasting Collecting the fluid into an EDTA tube allows for cell counts on the sample.
- 16. thoracentesis and laboratory analysis of the pleural fluid centrifugation of pleural fluid adding 1-2 ml of ethylether fluid stained with Sudan III
- 18. CT abdomen and thorax Lymphangiograph High fat content feed mixed with methylene blue
- 19. BIOCHEMICAL DIAGNOSIS OF CHYLOTHORAX pleural fluid triglyceride of >110 mg/dl had a 1% chance of being non-chylous and that a triglyceride of <50 mg/dl had a 5% chance of being chylous. As a result, pleural fluid triglyceride levels>1.24 mmol/l (110 mg/dl) with a cholesterol<5.18 mmol/l (200 mg/dl) is diagnostic of chylothorax
- 20. PSEUDOCHYLOTHORAX tuberculous pleurisy, chronic pneumothorax, rheumatoid pleurisy, poorly evacuated empyema and chronic haemothorax
- 22. Treatment is initially conservative: 1. Tube drainage. 2. Medium-chain fatty acid diet. 3. Fluid and electrolyte support. 4. NPO and TPN 5. Somatostatin Failure of conservative treatment requires surgical solution
- 23. OPERATIVE TECHNIQUES Direct ligation of thoracic duct Supradiaphragmatic mass ligation of the thoracic duct Video Assisted Thoracic Surgery (VATS) ‡‡Pleurodesis Fibrin glue
- 24. DIAGNOSTIC CONSIDERATIONS Timing of surgical management is controversial and depends on the etiology of the chylothorax and the patient's overall condition. Patients with postesophagectomy chylothorax have a 50-82% mortality rate if treated conservatively. A malignant etiology of the chylothorax must be ruled out, as greater than 50% of cases are due to malignancy, of which lymphoma accounts for approximately 75% of cases, followed by lung carcinoma.
- 25. ETIOLOGICAL TREATMENT sarcoidosis with steroids cardiac failure with diuretics Malignancy with radiotherapy or chemotherapy if no improvement then pleurodesis
- 26. If the leak is in the region of the neck or upper thorax, the thoracic duct is ligated in the area known as Poirier’s triangle between the arch of the aorta, internal carotid and vertebral column
- 27. Ligation of the thoracic duct is successful in 90% of patients when performed just above the right hemi-diaphragm
- 28. VATS FOR LIGATION OF THORACIC DUCT
- 29. THORACIC DUCT EMBOLIZATION -EMBOLIZATION PERFORMED BY COILS AND GELATIN SPONGE
- 30. too unfit for major surgery or have malignancy, a pleuroperitoneal shunt may be useful . complications such as infection, adhesions, and clogging of the implants 1% Evans blue dye can either be injected into the web space of the toes for uptake into the lymphatic space to increase visualization.
- 31. THANK U