Short case...Acute disseminated encephalomyelitis
•
2 j'aime•727 vues

Short case...Acute disseminated encephalomyelitis

Recommandé
Recommandé
Contenu connexe
En vedette
En vedette (20)
Similaire à Short case...Acute disseminated encephalomyelitis
Similaire à Short case...Acute disseminated encephalomyelitis (20)
Plus de Professor Yasser Metwally
Plus de Professor Yasser Metwally (20)
Dernier
Dernier (20)
Short case...Acute disseminated encephalomyelitis
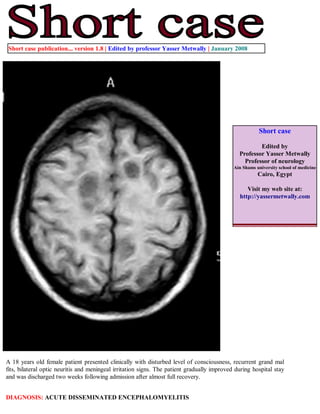
- 1. Short case publication... version 1.8 | Edited by professor Yasser Metwally | January 2008 Short case Edited by Professor Yasser Metwally Professor of neurology Ain Shams university school of medicine Cairo, Egypt Visit my web site at: http://yassermetwally.com A 18 years old female patient presented clinically with disturbed level of consciousness, recurrent grand mal fits, bilateral optic neuritis and meningeal irritation signs. The patient gradually improved during hospital stay and was discharged two weeks following admission after almost full recovery. DIAGNOSIS: ACUTE DISSEMINATED ENCEPHALOMYELITIS
- 2. Figure 1. Acute disseminated encephalomyelitis (ADEM). Postcontrast MRI T1 images showings scattered hypointense rounded and oval lesions, mostly situated at the junction of deep cortical gray and subcortical white matter. The immediate periventricular region is spared. Lesions are mostly larger than MS lesions and did not show contrast enhancement. Some lesions are seen encroaching upon the cortical grey matter. In general lesions did not have marked mass effect. Figure 2. Acute disseminated encephalomyelitis (ADEM). Postcontrast MRI T1 images showings scattered hypointense rounded and oval lesions, mostly situated at the junction of deep cortical gray and subcortical white matter. The immediate periventricular region is spared. Lesions are mostly larger than MS lesions and did not show contrast enhancement. Some lesions are seen encroaching upon the cortical grey matter. In general lesions did not have marked mass effect.
- 3. Figure 3. A case of acute disseminated encephalomyelitis. Notice that the multifocal cortical / subcortical hyperintense foci are sparing the periventricular region, and this is the classic pattern in ADEM. The foci, although of large size they have mild mass effect. Figure 4. Acute disseminated encephalomyelitis (ADEM). Notice that the multifocal cortical / subcortical lesions are sparing the periventricular region. The ADEM lesions are hypointense on MRI T1 images and hyperintense on MRI T2 and FLAIR images. ADEM lesions, though large, exert mild mass effect
- 4. Figure 5. Acute disseminated encephalomyelitis (ADEM). Notice that the multifocal cortical / subcortical lesions are sparing the periventricular region. The ADEM lesions are hypointense on MRI T1 images and hyperintense on MRI T2 and FLAIR images. ADEM lesions, though large, exert mild mass effect. DIFFERENTIAL DIAGNOSIS In the absence of specific biological markers, the diagnosis of ADEM is based upon clinical and imaging features. Clinical evaluation, neuroimaging, and blood and CSF analysis can help to distinguish ADEM from other conditions. [1] Herpes simplex encephalitis commonly presents with abnormal behavior and focal/secondary generalized seizures, which are more frequent and difficult to treat than in ADEM. MRI, EEG, and CSF polymerase chain reaction for Herpes simplex virus help in confirmation of the diagnosis. Japanese encephalitis presents with acute encephalopathy. MRI may show bilateral thalamic lesions, akin to ADEM. History, EEG findings, and CSF evidence of antibodies to the virus are useful for differentiation. Other infections such as bacterial meningitis and brain abscess can be ruled out by relevant investigations such as imaging and lumbar puncture. Complicated tuberculous meningitis may sometimes mimic ADEM and can be excluded if CSF sugar is normal and cultures are sterile. Neuromyelitis optica is characterized by optic neuritis and myelitis, with spinal lesions extending over three or more segments, features that may also be seen in ADEM. It may be distinguished from ADEM by the relative paucity of white matter lesions in MRI of the brain and presence of antibodies to aquaporin 4 (NMO-IgG). [1] Patients with Behcet's disease may present with multifocal neurological signs due to brain and spinal cord involvement. Clinical and imaging features may resemble ADEM, and the history of recurrent mucocutaneous ulcers of the mouth and genitalia will be essential to establish the diagnosis. Antiphospholipid antibody syndrome may also mimic the clinical and MRI features of ADEM and should be ruled out by measuring the specific antibodies. Immune-mediated disorders such as systemic lupus erythematosus, Sjögren syndrome, and sarcoidosis may present with neurological dysfunction and multifocal white matter changes and can be diagnosed by history and relevant blood tests. Susac's syndrome may present with subacute
- 5. encephalopathy, with MRI of the brain showing multiple white matter lesions; however, it can be differentiated from ADEM based on additional features such as the presence of headache, visual impairment due to retinal artery branch occlusion, sensorineural hearing loss, and specific involvement of central corpus callosum in MRI. [1] The diagnosis of recurrent ADEM should be made only after excluding other lesions such as arteriovenous malformations, neoplasms, and vasculitis. Metabolic leukoencephalopathies such as metachromatic leukodystrophy (MLD), adrenoleukodystrophy, and MELAS (mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes) may mimic childhood ADEM. Leukodystrophies may have a stepladder clinical course, with the exacerbations associated with febrile illnesses. History may reveal prior neurological dysfunction. MRI may show symmetric, confluent white matter lesions, hallmarks of inherited rather than acquired leukoencephalopathies. Specific investigations such as serum aryl sulfatase for MLD and very long-chain fatty acids (VLCFA) levels for adrenoleukodystrophy will confirm the diagnosis. The clinical features of mitochondrial cytopathies such as MELAS may be similar to that of ADEM and lesions seen on MRI may be transient. Serum and CSF lactate levels may be elevated during the acute episode and MR spectroscopic imaging may show elevated lactate in the affected tissues. [1] ADEM or multiple sclerosis? In a patient presenting with neurological dysfunction and MRI showing multiple white matter lesions, the most important differential diagnosis is MS. Distinguishing between ADEM and MS is a diagnostic challenge and has important therapeutic and prognostic implications. There are several clinical, imaging, and laboratory parameters that may be useful to distinguish between the two. CSF electrophoresis has shown a significant reduction in the beta-1 globulin fraction in patients with MS as compared to those with ADEM and this may be a potential CSF marker. [1] Features that strongly favor ADEM include a history of preceding infection, polysymptomatic neurological dysfunction, encephalopathy, grey matter involvement on MRI, and absence of oligoclonal bands in CSF. Often, distinction between these two conditions cannot be made with certainty and follow-up with serial MRI may be necessary to establish the diagnosis. Addendum A new version of this software is uploaded in my web site every week (every Saturday and remains available till Friday.) To download the current version follow the link quot;http://pdf.yassermetwally.com/short.pdfquot;. You can download the long case version of this short case during the same week from: http://pdf.yassermetwally.com/case.pdf or visit web site: http://pdf.yassermetwally.com To download the software version of the publication (crow.exe) follow the link: http://neurology.yassermetwally.com/ crow.zip At the end of each year, all the publications are compiled on a single CD-ROM, please contact the author to know more details. Screen resolution is better set at 1024*768 pixel screen area for optimum display References 1. Metwally, MYM: Textbook of neurimaging, A CD-ROM publication, (Metwally, MYM editor) WEB-CD agency for electronic publishing, version 9.1a January 2008