Adolescent Reproductive Health_Cate Lane_5.6.14

Three interventions are proven ineffective for improving adolescent sexual and reproductive health: 1. Youth centers do not effectively deliver sexual health services and have high costs per beneficiary. 2. Peer education alone shows limited effects on behaviors and health outcomes, with greatest impact on peer educators. 3. Child marriage legislation has limited impact, as rates decline for other reasons beyond legal reforms. Two effective interventions are comprehensive sexuality education, which is most effective when curricula are developed through participatory processes and address knowledge, attitudes and skills. Adolescent friendly health services also increase utilization when providers are non-judgemental, facilities are appealing, and communities are engaged. A focus on positive youth development through skills, participation, relationships and

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
Similaire à Adolescent Reproductive Health_Cate Lane_5.6.14
Similaire à Adolescent Reproductive Health_Cate Lane_5.6.14 (20)
Plus de CORE Group
Plus de CORE Group (20)
Dernier
Dernier (20)
Adolescent Reproductive Health_Cate Lane_5.6.14
- 1. Programs for Adolescent Sexual and Reproductive Health: What Works? May 1 2014 Cate Lane, Youth Advisor USAID/GH/PRH
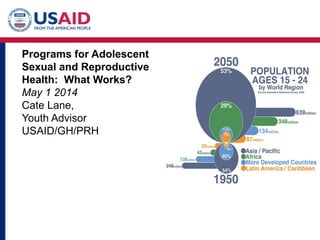
- 2. Defining 1.8 billion Youth . •Around 1 in 4 persons is an adolescent aged 10- 24 •In all developing countries, youth are about 29 percent of the total population •There will be about 72 million more youth in 2025 than there are today •About 16 million girls aged 15 to 19 years and two million girls under the age of 15 give birth every year. The majority of these births occur within marriage. •More than 30% of girls in developing countries are married before age 18, with 14% married before age 15.
- 3. Insanity: doing the same things over and over and expecting different results Albert Einstein Around the world: Ineffective interventions intended to improve adolescent sexual and reproductive health (ASRH) continue be implemented; Effective interventions are not replicated with attention to those attributes that contribute to their effectiveness As a result: There are no observed health behaviour changes nor beneficial outcomes for youth Questions are raised about the value of ASRH policies and programs Human and financial resources are used that could be deployed elsewhere Three interventions are proven to be ineffective in improving adolescent sexual and reproductive health, yet continue to be implemented.
- 4. YOUTH CENTERS • Youth centers are meeting points that offer a youth- friendly, safe, non- threatening environment for information and service provision.
- 5. 1. Youth centers are not effective in delivering sexual and reproductive health services for adolescents. 2. An evaluation of 18 youth centre programs showed: – Older male youths who live nearby used the services, mainly for recreation – There were no or limited effects on the use of sexual and reproductive health services or commodities – The cost per beneficiary was very high YOUTH CENTERS – What have we learned?
- 6. PEER EDUCATION: A Popular Approach • Peer education is popular because (theoretically): – It makes use of existing social networks, information exchange and open discussion between adolescents of similar age and social status – It provides opportunities for regular contact in a friendly context – It may be more successful at getting to hard to reach youth over traditional adult- led health-education approaches
- 7. PEER EDUCATION – What have we learned? Five meta-analyses of peer education program implemented over many years in different contexts conclude that peer education programs show limited effects in promoting safe behaviours and in improving health, on their own. Greatest impact is often among the peer educators themselves “Peer education might be more effective if it is integrated in holistic interventions and if the role of peer educators is redefined in a way that makes them more of a source of sensitization and referral to experts and services.” Source: 1. Harden A, Oakley A, Oliver S. Peer-delivered health promotion for young people: A systematic review of different study designs. Health Education Journal. 2001; 60(4):339-353. 2. Medley A, Kennedy C, O'Reilly K, Sweat M. Effectiveness of peer education interventions for HIV prevention in developing countries: A systematic review and meta-analysis. AIDS Education and Prevention. 2009; 21(3):181-206. 3. Kim CR, Free C. Recent evaluations of the Peer Led approach in adolescent sexual health education: A systematic review.‐ Perspectives on sexual and reproductive health. 2008; 40(3):144-151. 4. Maticka-Tyndale E, Barnett JP. Peer-led interventions to reduce HIV risk of youth: A review. Evaluation and Program Planning. 2010;33(2):98-112. 5. Tolli M. Effectiveness of peer education interventions for HIV prevention, adolescent pregnancy prevention and sexual health promotion for young people: A systematic review of European studies. Health Education Research. 2012;27(5):904-913.
- 8. CHILD MARRIAGE •A widespread harmful practice that affects enormous numbers of girls. One third of the world’s girls are married before the age of 18 and 1 in 9 are married before the age of 15. In 2010, 67 million aged 20-24 were married before age 18. If present trends continue, an average of 14.2 million girls will marry each year. •Countries with the highest prevalence of child marriage are concentrated in Western and Sub-Saharan Africa, but the largest number of child brides reside in South Asia. •Early marriage is linked to early childbearing, which has numerous and serious consequences for the health and well- being of girls and their babies.
- 9. CHILD MARRIAGE – what have we learned? • The contribution of legislation to change the practice has been very limited. • There is little correlation between legislation and trends • There are very few indications that laws and legal reforms have contributed to discouraging and eradicating child marriage. • Among the 12 African countries that have had more than 10% decrease in general, only three countries are considered to have a strong legal framework (Ethiopia, Liberia, Sierra Leone). • In the few countries with declining rates it is not possible to ascribe the changes to legal reforms or legal mechanisms. Source: 1. J Svanemyr, E Scolaro, K Blondeel, V Chandra-Mouli, M Temmerman. The contribution of laws to change the practice of child marriage in Africa. 2013. Paper prepared by WHO for the Inter-Parliamentary Union. 2. S Lee-Rife, A Malhotra, A Warner, A McGonagle Glinski. What works to prevent child marriage: A review of the evidence. Studies in Family Planning. 2012. 43, 4, 287-303.
- 10. Soooo, what DOES work? • Two interventions have proven to be effective but are often executed with little attention to those key attributes that contribute to their effectiveness.
- 11. COMPREHENSIVE SEXUALITY EDUCATION Age-appropriate, culturally relevant approach to teaching about sex and relationships by providing scientifically accurate, realistic, non-judgmental information. Source: UNESCO, UNAIDS, UNFPA, UNICEF and WHO. International technical guidance on sexuality education. Volume 1. The rationale for sexuality education. An evidence-informed approach for schools, teachers and health educators. UNESCO. Paris. 2009.
- 12. COMPREHENSIVE SEXUALITY EDUCATION: what makes it effective? Common characteristics that effectively increase knowledge, clarify values and attitudes, increase skills and affect behaviour include: 1.The process of developing the curriculum 2.The content of curriculum itself 3.The manner in which it is delivered Source: UNESCO, UNAIDS, UNFPA, UNICEF and WHO. International technical guidance on sexuality education. Volume 1. The rationale for sexuality education. An evidence-informed approach for schools, teachers and health educators. UNESCO. Paris. 2009.
- 13. To be considered adolescent-friendly, health services should be: Accessible •Adolescents are able to obtain the health services that are available Acceptable •Adolescents are willing to obtain the health services that are available Equitable •All adolescents, not just some groups of adolescents, are able to obtain the health services that are available Appropriate •The right health services (i.e. the ones they need) are provided to them Effective •The right health services are provided in the right way, and make a positive contribution to their health Source: WHO. Making health services adolescent friendly. Developing national quality standards. WHO. Geneva. 2013. ADOLESCENT FRIENDLY HEALTH SERVICES
- 14. ADOLESCENT FRIENDLY HEALTH SERVICES – What works? Health services have been shown to increase utilization of health services by adolescents only if they have all four of these characteristics: 1.Health service providers are trained and supported to be non judgemental and friendly in their dealings with adolescents 2.Actions are taken to make health facilities welcoming and appealing to adolescents 3.Communication with adolescents to inform them about the availability of ‘friendly’ health services and to encourage them to use the services when needed 4.Communication with community members to make them aware of the importance of providing adolescents with health services
- 15. New Ways of Thinking: Prevention vs Treatment • Most common approach globally to youth reproductive health has focused on the treatment of adolescent problems, • Growing evidence base of methodologies that prevent or moderate problems and consequences before they occur
- 16. New Understanding: The Adolescent Brain
- 17. SKILL-BUILDING: Intentional focus on broadening youth perspectives; development of social, problem-solving and communication skills; PARTICIPATION: Engaging and partnering with youth by offering meaningful and developmentally appropriate opportunities for participation (e.g., youth-led discussion, real choices) and leadership (e.g., youth as peer counselors, tutors, evaluators, and contributors) MEMBERSHIP: Creating a sense of membership and/or a sense of commitment to school, workplace, culture, and community NORMS AND EXPECTATIONS: Establishing norms and high expectations for positive youth behavior and action that are sanctioned by the group ADULT-YOUTH RELATIONSHIPS: Establishing deep and meaningful ways for young people and adults to relate and engage with each other and specific training for adult leaders INFORMATION AND SERVICES: Providing problem-specific information and access to developmentally appropriate services Source: Developed by the Academy for Educational Development, derived from Eccles and Gootman, eds. (2002). Community Programs to Promote Youth Development . National Academies of Science. Greater attention to Positive Youth Development Principles
- 18. Thank you! Resources for ASRH programming: • IYWG.org