
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à P wave (ECG) - Dr. Akif Baig
Similaire à P wave (ECG) - Dr. Akif Baig (20)
Plus de akifab93
Plus de akifab93 (20)
Dernier
Dernier (20)
P wave (ECG) - Dr. Akif Baig
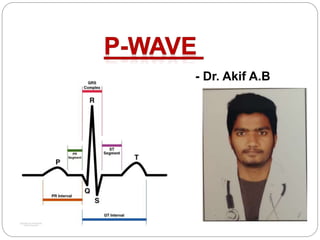
- 1. - Dr. Akif A.B
- 4. P Wave The P wave is the first positive deflection on the ECG It represents atrial depolarisation Normal duration: < 0.12 s (< 120ms or 3 small squares)
- 5. Characteristics of the Normal Sinus P Wave Morphology Smooth contour Monophasic in lead II Biphasic in V1 Duration < 0.12 s (<120ms or 3 small squares) Amplitude < 2.5 mm (0.25mV) in the limb leads < 1.5 mm (0.15mV) in the precordial leads Atrial abnormalities are most easily seen in the inferior leads (II, III and aVF) and lead V1, as the P waves are most prominent in these leads
- 6. Normal P-wave Morphology – Lead II The right atrial depolarisation wave (brown) precedes that of the left atrium (blue) The combined depolarisation wave, the P wave, is less than 120 ms wide and less than 2.5 mm high
- 7. Normal P-wave Morphology – Lead V1 The P wave is typically biphasic in V1, with similar sizes of the positive and negative deflections
- 8. Inverted P Waves P-wave inversion in the inferior leads indicates a non-sinus origin of the P waves When the PR interval is < 120 ms, the origin is in the AV junction (e.g. accelerated junctional rhythm)
- 10. When the PR interval is ≥ 120 ms, the origin is within the atria (e.g. ectopic atrial rhythm)
- 11. MULTIFOCAL ATRIAL RHYTHM The presence of multiple P wave morphologies indicates multiple ectopic pacemakers within the atria and/or AV junction If ≥ 3 different P wave morphologies are seen, then multifocal atrial rhythm is diagnosed
- 12. MULTIFOCAL ATRIAL TACHYCARDIA If ≥ 3 different P wave morphologies are seen and the rate is ≥ 100, then multifocal atrial tachycardia (MAT) is diagnosed
- 14. Right Atrial Enlargement – Lead II In right atrial enlargement, right atrial depolarisation lasts longer than normal and its waveform extends to the end of left atrial depolarisation Although the amplitude of the right atrial depolarisation current remains unchanged, its peak now falls on top of that of the left atrial depolarisation wave The combination of these two waveforms produces a P waves that is taller than normal (> 2.5 mm), although the width remains unchanged (< 120 ms)
- 15. ECG Criteria of Right Atrial Enlargement Right atrial enlargement produces a peaked P wave (P pulmonale) with amplitude: > 2.5 mm in the inferior leads (II, III and AVF) > 1.5 mm in V1 and V2
- 17. Causes of Right Atrial Enlargement The principal cause is pulmonary hypertension due to: Chronic lung disease (cor pulmonale) Tricuspid stenosis Congenital heart disease (pulmonary stenosis, Tetralogy of Fallot) Primary pulmonary hypertension
- 18. • Right atrial enlargement: P pulmonale • P wave amplitude > 2.5mm in leads II, III and aVF
- 19. Right atrial enlargement: P wave amplitude > 1.5 mm in V1 and V2
- 21. Left atrial enlargement (LAE) is due to pressure or volume overload of the left atrium LAE is often a precursor to atrial fibrillation
- 22. Left Atrial Enlargement – Lead II Left atrial depolarisation lasts longer than normal but its amplitude remains unchanged Therefore, the height of the resultant P wave remains within normal limits but its duration is longer than 120 ms A notch (broken line) near its peak may or may not be present (“P mitrale”)
- 23. P wave changes with Left Atrial Enlargement
- 24. ECG Criteria for Left Atrial Enlargement LAE produces a broad, bifid P wave in lead II (P mitrale) and enlarges the terminal negative portion of the P wave in V1. In lead II Bifid P wave with > 40 ms between the two peaks Total P wave duration > 110 ms
- 25. In V1 Biphasic P wave with terminal negative portion > 40 ms duration Biphasic P wave with terminal negative portion > 1mm deep
- 26. Causes of left atrial hypertrophy In isolation: Classically seen with mitral stenosis In association with left ventricular hypertrophy Systemic hypertension Aortic stenosis Mitral incompetence Hypertrophic cardiomyopathy
- 28. Biatrial Enlargement Definition Biatrial enlargement is diagnosed when criteria for both right and left atrial enlargement are present on the same ECG The diagnosis of biatrial enlargement requires criteria for LAE and RAE to be met in either lead II, lead V1 or a combination of leads
- 29. ECG Criteria for Biatrial Enlargement In lead II Bifid P wave with Amplitude ≥ 2.5mm AND Duration ≥ 120 ms In V1 Biphasic P waves with Initial positive deflection ≥ 1.5mm tall AND Terminal negative deflection ≥ 1mm deep AND Terminal negative deflection ≥ 40 ms duration
- 30. Biphasic P waves in V1 with a very tall positive deflection (almost 3 mm in height) and a negative deflection that is both deep (> 1 mm) and wide (> 40 ms)
- 31. Biatrial enlargement: • P waves in lead II are tall (> 2.5mm) and wide (> 120 ms) • P waves in V2 are tall (> 1.5 mm), while the terminal negative portion of V1 is deep (> 1mm) and wide (> 40 ms)
- 32. For more videos, do subscribe to my Youtube Channel – Dr. Akif Baig