Contenu connexe
Similaire à Hiperkalemia (20)
Hiperkalemia
- 1. NATURE REVIEWS | NEPHROLOGY ADVANCE ONLINE PUBLICATION | 1
University of Tennessee
Health Science Center,
University of Tennessee,
956 Court Avenue,
Memphis, TN 38163,
USA.
csaba.kovesdy@va.gov
Management of hyperkalaemia in chronic
kidney disease
Csaba P. Kovesdy
Abstract | Hyperkalaemia is common in patients with chronic kidney disease (CKD), in part because of the
effects of kidney dysfunction on potassium homeostasis and in part because of the cluster of comorbidities
(and their associated treatments) that occur in patients with CKD. Owing to its electrophysiological effects,
severe hyperkalaemia represents a medical emergency that usually requires prompt intervention, whereas
the prevention of hazardous hyperkalaemic episodes in at-risk patients requires measures aimed at the long-
term normalization of potassium homeostasis. The options for effective and safe medical interventions to
restore chronic potassium balance are few, and long-term management of hyperkalaemia is primarily limited
to the correction of modifiable exacerbating factors. This situation can result in a difficult trade-off in patients
with CKD, because drugs that are beneficial to these patients (for example, renin–angiotensin–aldosterone-
system antagonists) are often the most prominent cause of their hyperkalaemia. Maintaining the use of these
beneficial medications while implementing various strategies to control potassium balance is desirable;
however, discontinuation rates remain high. The emergence of new medications that specifically target
hyperkalaemia could lead to a therapeutic paradigm shift, emphasizing preventive management over ad hoc
treatment of incidentally discovered elevations in serum potassium levels.
Kovesdy, C. P. Nat. Rev. Nephrol. advance online publication 16 September 2014; doi:10.1038/nrneph.2014.168
Introduction
Hyperkalaemia is one of the clinically most important
electrolyte abnormalities because it can cause severe
electrophysiological disturbances, such as cardiac arrhyth
mias. Hyperkalaemia is defined as a serum potassium level
above the normal range, and various arbitrary cutoffs,
such as >5.0, >5.5 or >6.0 mmol/l, are used to denote dif
ferent levels of severity. Hyperkalaemia has been associ
ated with increased mortality in patients with chronic
kidney disease (CKD) and those undergoing haemo
dialysis,1–4
highlighting the importance of maintaining
serum potassium levels in the physiologically normal
range. The mechanisms driving hyperkalaemia typically
involve a combination of factors, such as increased dietary
potassium intake, disordered distribution between intra
cellular and extracellular compartments and abnormali
ties in potassium excretion. In clinical practice, CKD is the
most common predisposing condition for hyperkalaemia
and, in combination with one or more exacerbating
factors (discussed below), can induce recurrent episodes
of abnormally elevated serum potassium levels.
Hyperkalaemia occurs especially frequently in patients
with CKD who are treated with certain classes of medi
cations, such as angiotensin-converting-enzyme (ACE)
inhibitors, angiotensin-receptor blockers (ARBs) or
other inhibitors of the renin–angiotensin–aldosterone
system (RAAS). These therapeutic agents are beneficial
in patients with CKD and are also the standard of care
for some common comorbidities of CKD, such as con
gestive heart failure (CHF). Although treatment with
RAAS inhibitors is desirable in patients with CKD, it
is often difficult or impossible to continue this therapy
over extended periods of time owing to the development
of hyperkalaemia. Currently, no reliably effective and
safe maintenance treatments can be given in combina
tion with RAAS inhibitors to offset the hyperkalaemia
caused by these otherwise beneficial therapeutic agents.
Hence, the safe response to recurrent episodes of hyper
kalaemia in patients with CKD who receive RAAS inhib
itors is considered to be tapering or discontinuation of
this medication.
This Review summarizes the mechanisms under
lying hyperkalaemia, its epidemiology and clinical
consequences, with a focus on patients with CKD and end-
stage renal disease (ESRD). Currently available treatment
regimens are discussed, highlighting areas of uncertainty,
and emerging therapies that might enable the more-liberal
use of RAAS inhibitors in various populations of patients
at risk of hyperkalaemia are described.
Mechanisms of hyperkalaemia in CKD
The principal mechanism through which the kidneys
maintain potassium homeostasis is the secretion of
potassium into the distal convoluted tubule and the prox
imal collecting duct. As glomerular filtration rate (GFR)
decreases, the ability of the kidneys to maintain serum
potassium levels in a physiologically normal range is
increasingly jeopardized.5–9
Experimental studies suggest
Competing interests
The author declares no competing interests.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved
- 2. 2 | ADVANCE ONLINE PUBLICATION www.nature.com/nrneph
that the kidneys can adjust to a decrease in the number
of nephrons through increasing potassium secretion by
the surviving nephrons, and remain able to maintain
normokalaemia under steady state conditions. However,
their ability to respond to an acute increase in potas
sium load is hampered, resulting in the development of
hyperkalaemic episodes.10
Patients with CKD often have other conditions that
exacerbate hyperkalaemia, in addition to the decreased
GFR and tubulointerstitial damage that prevent the
kidneys from upregulating potassium excretion
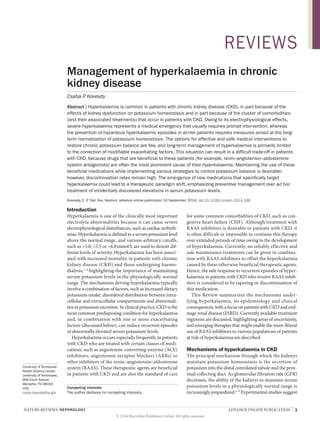
(Figure 1). Often, multiple precipitating factors are
present in a single patient, which explains why hyper
kalaemia is most commonly detected in patients with
CKD in clinical practice. Dietary modifications in patients
with CKD often involve an emphasis on sodium restric
tion, and some patients switch to salt substitutes, not real
izing that these can contain potassium salts. Furthermore,
‘heart-healthy’ diets are inherently rich in potassium—
which is beneficial in most people (by virtue of improved
blood pressure control and other mechanisms), but can
also contribute to an increased risk of hyperkalaemia in
susceptible patients. Other CKD-related conditions that
contribute to hyperkalaemia are metabolic acidosis, which
causes a shift of potassium from the intracellular to the
extracellular space11
(the effect of which depends more
on the aetiology of the acidosis rather than on the actual
pH);12–15
anaemia requiring blood transfusion, which can
result in a high acute potassium load (typically occurring
with large transfusions and the use of outdated blood);16
and kidney transplantation, which can result in hyper
kalaemia through various mechanisms (for example,
development of renal tubular acidosis or the effects of
calcineurin inhibitors).17–19
In addition, some hyperkalaemia-inducing comorbid
ities are not caused by CKD itself, but often occur in
patients with CKD, and hence are instrumental to the
high incidence of hyperkalaemia seen in these patients.
Acute kidney injury results in a rapid decrease in both
GFR and tubular flow, and is often accompanied by a
hypercatabolic state, tissue injury and high acute potas
sium loads (for example, secondary to gastrointestinal
bleeding). These conditions all contribute to the develop
ment of hyperkalaemia, which can be of life-threatening
severity and is one of the most common indications
for emergency haemodialysis. Diabetes mellitus and
cardiovascular disease are two of the most common
comorbidities in patients with CKD and both are linked
to the development of hyperkalaemia through differ
ent mechanisms. Insulin deficiency and hypertonicity
caused by hyperglycaemia in patients with diabetes con
tributes to an inability to disperse high acute potassium
loads into the intracellular space.20
Furthermore, dia
betes mellitus is associated with hyporeninaemic hypo
aldosteronism and the resultant inability to upregulate
tubular potassium secretion.21,22
Cardiovascular disease and other associated condi
tions, such as acute myocardial ischaemia, left ventricular
hypertrophy and CHF, require various medical treatments
that have been linked to hyperkalaemia (Figure 1). Their
importance in the aetiology of hyperkalaemia in patients
with CKD is underscored by the fact that some of these
medications are difficult or impossible to use in patients
with CKD who are, therefore, deprived of their proven
cardiovascular benefits. For example, β2
-adrenergic-
receptor blockers contribute to hyperkalaemia through
inhibition of renin production and a decreased ability
to redistribute potassium to the intracellular space.23
Heparin treatment has also been linked to hyperkalaemia
through decreased production of aldosterone.24
Cardiac
glycosides, such as digoxin, contribute to hyperkalaemia
through inhibition of the Na+
/K+
-ATPase, which is neces
sary for secretion of potassium into the collecting duct and
for redistribution of potassium across cell membranes.25
However, the effects of these drugs on serum potassium
levels are limited (increases of ~0.2–0.5 mmol/l) unless
other predisposing factors are present.26,27
The medications linked to hyperkalaemia that are
most relevant in clinical practice are RAAS inhibitors
(ACE inhibitors, ARBs, direct renin inhibitors and
mineralocorticoid-receptor blockers). In populations
without CKD, the incidence of hyperkalaemia associated
with RAAS inhibitor monotherapy is 2%. However, the
incidence of hyperkalaemia increased to 5% in patients
receiving dual-agent RAAS inhibitor therapy, and to
5–10% when dual therapy was administered to patients
with CKD (Table 1).28,29
Hyperkalaemia is perhaps the
most important cause of the intolerance to RAAS inhibi
tors observed in a substantial proportion of patients with
CKD. In clinical trials of ACE inhibitors, hyperkalaemia
led to discontinuation of the study drug in 1.2–1.6% of
patients,28
but the discontinuation rate is probably much
higher in routine clinical practice, in which these drugs
are prescribed to a nonselected population of patients.
The fact that RAAS inhibitors are poorly tolerated in
patients with CKD is especially critical as treatment
with these agents is associated with mortality benefits30,31
and, perhaps even more importantly, they represent one
of the very few therapeutic interventions with proven
renoprotective effects available in clinical practice.
Epidemiology of hyperkalaemia in CKD
Frequency
The incidence and prevalence of hyperkalaemia in the
general population is low (2–3%).32–34
However, studies in
patients with CKD have found notably higher frequencies
Key points
■■ Hyperkalaemia is common in patients with chronic kidney disease (CKD),
especially when CKD is accompanied by exacerbating factors
■■ Hyperkalaemia is associated with adverse outcomes in patients with CKD,
and can restrict the use of beneficial medications, such as renin–angiotensin–
aldosterone-system (RAAS) inhibitors
■■ Current therapeutic paradigms for hyperkalaemia emphasize intermittent
acute interventions and the elimination of exacerbating factors (including
RAAS inhibitors)
■■ Proactive treatment strategies to prevent the development of hyperkalaemia
could also benefit patients by enabling more liberal use of RAAS inhibitors
■■ The emergence of new potassium binders may result in more widespread
implementation of strategies for hyperkalaemia prevention
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved
- 3. NATURE REVIEWS | NEPHROLOGY ADVANCE ONLINE PUBLICATION | 3
of hyperkalaemia—often as high as 40–50%—especially
in diabetic patients, those with advanced stages of
CKD,3,33,35
kidney transplant recipients17
and patients
treated with RAAS inhibitors.36,37
The strong association
of RAAS inhibitor therapy with hyperkalaemia is further
underscored by the results of clinical trials of these agents
in patients with CKD. Early clinical trials did not report
the incidence of hyperkalaemia, and discontinuation
rates related to this complication were very low (typically
1–2%).38–42
In subsequent trials, however, the incidence
of hyperkalaemia ranged from 1.9% to 38.4%; hyper
kalaemia was most common in patients with advanced
CKD and its incidence increased with the number of
RAAS inhibitors received (Table 1).38–48
Differences in
reported rates of hyperkalaemia between clinical trials
could relate to different definitions of hyperkalaemia, dif
ferent patient populations, or occur because some trials
required confirmation of hyperkalaemia by repeat meas
urements. As in the early clinical trials, treatment dis
continuation rates due to hyperkalaemia remain very low
in contemporary studies. However, the strict enrolment
criteria and close follow-up of patients included in clinical
trials mean that these reported rates of hyperkalaemia and
treatment discontinuation due to hyperkalaemia probably
greatly underestimate the real frequency of these events
in everyday clinical practice.49,50
The success of RAAS
inhibitors in achieving improved clinical outcomes and
the apparent absence of hyperkalaemia as an important
problem in clinical trials has resulted in increased use of
these agents in patients who would have been excluded
from these trials because of, for example, more-advanced
CKD or high baseline serum potassium levels. This situ
ation might have contributed to the marked increase in
hyperkalaemia rates seen in everyday practice following
the publication of some influential RAAS inhibitor trials
and to a worrisome increase in hyperkalaemia-related
morbidity and mortality.51
Interestingly, in one study, the
incidence of hyperkalaemia seemed to increase following
the initiation of RAAS inhibitors even in patients receiv
ing maintenance dialysis, although the lack of functioning
kidneys in these patients should have rendered them
immune to hyperkalaemia caused by RAAS inhibitors.
These observations might be attributable to the inhibitory
effects of these agents on both gastrointestinal and renal
tubular potassium excretion in patients with residual
kidney function.52
Moreover, the results of small pub
lished53–58
and ongoing59
clinical trials in the past 5 years
suggest that mineralocorticoid-receptor blockers, such
as spironolactone or eplerenone, have beneficial effects
in patients on dialysis. Use of these agents could, there
fore, increase and result in a rise in hyperkalaemia rates
in patients on dialysis.
Outcomes
Hyperkalaemia is associated with increased mortality
in patients with normal kidney function as well as in
patients along the entire spectrum of CKD severity. The
effects of hyperkalaemia are mediated through complex
Hyperkalaemia
Acute
kidney
injury
Inability to secrete
or excrete K+
High acute
K+
load
K+
shift into
extracellular space
Renal tubular acidosis or effects
of calcineurin inhibitors
Anaemia requiring
blood transfusion
Metabolic
acidosis
Chronic
kidney
disease
Tubulointerstitial
damage
Decreased
GFR
Dietary
modifications
Inhibition of
Na+
/K+
-ATPase:
decreased ductal
K+
reabsorption
and K+
redistribution across
cell membranes
Decreased renin
production:
decreased
ability to
redistribute
K+
to the
intracellular space
Inability to induce
tubular K+
secretion
Hypertonicity
Hyporeninaemic
hypoaldosteronism
Diabetes
mellitus
Cardiovascular disease
including acute
myocardial ischaemia,
left ventricular hypertrophy
and congestive heart failure
RAAS
inhibitors
Mineralo-
corticoid-
receptor
blockers
Block of
aldosterone
effects:
decreased
K+
secretion
Cardiac
glycosidesHeparin
β2
-receptor
antagonists
Increased dietary
K+
intake
Tissue
injury
Decreased
urine flow
Kidney
transplantation
Inability to dispose
of K+
into the
intracellular space
Relative
insulin
deficiency
Decreased
production
of aldosterone:
decreased
K+
secretion
Figure 1 | Mechanisms contributing to the development of hyperkalaemia in patients with chronic kidney disease and
associated comorbidities. Abbreviations: GFR, glomerular filtration rate; RAAS, renin–angiotensin–aldosterone system.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved
- 4. 4 | ADVANCE ONLINE PUBLICATION www.nature.com/nrneph
alterations in cell membrane electrophysiology,60,61
a detailed description of which is beyond the scope of this
Review. Studies in patients with non-dialysis-dependent
CKD demonstrated a significant association between
hyperkalaemia and increased long-term all-cause mor
tality.3,62
Similar associations between hyperkalaemia
and mortality were reported in patients receiving chronic
haemodialysis,1,2,4
but assessment of the increased mor
tality attributable to hyperkalaemia in this population is
confounded by exposure to low-potassium dialysates,
which are themselves a risk factor for sudden death.63,64
In patients receiving peritoneal dialysis, hyperkalaemia
and variability in serum potassium levels were associated
with increased mortality in the first year following the
measurement of an abnormal potassium level, but not
thereafter.65
This discrepancy between the short-term and
long-term associations with mortality could be explained
by the electrophysiological effects of hyperkalaemia,
which present an acute danger primarily because they can
cause cardiac arrhythmias.66–68
Indeed, studies that exam
ined mortality associated with abnormal serum potassium
levels during a short time-window have corroborated the
existence of this short-term mortality risk.33
Treatment of hyperkalaemia
Acute management
It is unclear what level of hyperkalaemia represents an
imminent danger to the individual. In a large retrospec
tive study, a serum potassium level 6 mmol/l was associ
ated with a greater than 30-fold increase in the risk of
1‑day mortality,33
but long-term adverse effects of hyper
kalaemia have been associated with levels 5 mmol/l.45
It
is important to emphasize that, beside the absolute serum
potassium level, numerous other factors determine when
hyperkalaemia becomes hazardous in a given individual,
such as the rate of change in serum potassium levels, the
concurrent presence of low serum concentrations of
calcium and magnesium (often exacerbated by the use
of diuretics and/or proton pump inhibitors) or abnormal
serum pH. To what extent the concomitant presence of
such abnormalities might potentiate the electrophysio
logical effects of hyperkalaemia is not well established
and needs further examination. Severe hyperkalae
mia (most often defined as serum levels 6 mmol/l)
typically represents a clinical urgency or emergency,
which may warrant immediate attention in the form of
cardiac monitoring, acute medical interventions and,
occasionally, emergency dialysis.
Diagnostic electrocardiography
In the acute management of hyperkalaemia, electro
cardiography (ECG) is often used to gauge the sever
ity of its effect on cardiac function. However, individual
variations in sensitivity to serum levels of potassium are
evident in the ECG changes typically associated with
hyperkalaemia, such as peaked T waves, as well as pro
longation of the PR interval and QRS complex duration.
Although case reports in patients with serum potassium
levels 9 mmol/l highlight an association with marked
ECG changes,69–71
the ability of ECG features to predict
hyperkalaemia of moderate severity is considered poor,
since only half of patients with serum potassium levels
6.5 mmol/l display typical ECG changes.72
In a retro
spective study of 90 patients with hyperkalaemia (of
whom 80% had serum potassium levels 7.2 mmol/l),
typical ECG changes associated with hyperkalaemia
showed poor sensitivity and specificity for predicting
patients’ actual serum potassium levels,73
prompting
the authors to recommend that these ECG changes
should not be used to guide treatment of hyperkalaemia.
In another study of 145 patients with ESRD, the ratio
of T wave to R wave amplitude was more specific than
T wave tenting for predicting a serum potassium level
6 mmol/l, but both features had poor sensitivity (33%
Table 1 | Hyperkalaemia associated with RAAS inhibitor use in selected clinical trials in patients with CKD
Study (year
main results
published)
Patients receiving RAAS inhibitor Definition of
hyperkalaemia
Incidence Discontinuation due
to hyperkalaemia
RENAAL45
(2001)
675 patients with diabetic nephropathy
and sCr 115–265 μmol/l
≥5.0 mmol/l and
≥5.5 mmol/l
38.4% (≥5.0 mmol/l)
10.8% (≥5.5 mmol/l)
Not reported
IDNT47
(2001)
579 patients with diabetic nephropathy
and sCr 88.40–265.00 μmol/l
6 mmol/l 18.6% 2.1% (irbesartan)
0.4% (placebo)
J-LIGHT44
(2004)
58 Japanese patients with sCr
180.34 ± 42.43 μmol/l*
5.1 mmol/l 5.2% Not reported
Benazepril in
advanced CKD48
(2006)
226 Chinese patients with advanced CKD
Group 1: eGFR 37.10 ± 6.30 ml/min/1.73 m2
*
Group 2: eGFR 26.30 ± 5.30 ml/min/1.73 m2
*
≥6.0 mmol/l 1.9% (group 1)
5.3% (group 2)
1.3% (3 patients
from group 2)‡
AASK43
(2009)
417 African American patients with eGFR
46.30 ± 13.50 ml/min/1.73 m2
*
5.5 mmol/l 7.2% Not reported
NEPHRON‑D46
(2013)
1,448 US veterans (99% men) with diabetic
nephropathy and eGFR 30–90 ml/min/1.73 m2
6.0 mmol/l, or need
for emergency room
visit, hospitalization
or dialysis
4.4%
(losartan + placebo)
9.9%
(losartan + lisinopril)
Not reported
*Values are ± 1 SD. ‡
Unclear in which treatment arm. Abbreviations: AASK, African American Study of Kidney Disease and Hypertension; CKD, chronic kidney
disease; eGFR, estimated glomerular filtration rate; IDNT, Irbesartan Diabetic Nephropathy Trial; J‑LIGHT, Japanese Losartan Therapy Intended for the Global
Renal Protection in Hypertensive Patients; NEPHRON‑D, Veterans Affairs Nephropathy in Diabetes; RAAS, renin–angiotensin–aldosterone system; RENAAL,
Reduction of Endpoints in Noninsulin-Dependent Diabetes Mellitus with the Angiotensin II Antagonist Losartan; sCr, serum creatinine.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved
- 5. NATURE REVIEWS | NEPHROLOGY ADVANCE ONLINE PUBLICATION | 5
and 24%, respectively).74
Interestingly, patients in this
study who had an abnormal T:R wave amplitude ratio
had an increased long-term risk of sudden death, sug
gesting that ECG changes might identify patients who
are particularly sensitive to the electrophysiological
effects of hyperkalaemia.74
In response to the publica
tion of this study, other researchers commented75
that
intravenous infusion of calcium into hyperkalaemic
patients with ECG changes linked to hyperkalaemia
could serve as a test to determine whether these changes
were incidental to or caused by the hyperkalaemia, and
whether treatment of hyperkalaemia could be expected
to reverse them.75
Interventions
Interventions used to treat acute hyperkalaemia include
the intravenous administration of either calcium salts
or hypertonic saline (which is effective in patients with
underlying hyponatraemia).76,77
These agents restore
the electrophysiological properties of cell membranes
through various mechanisms,78–83
but do not (or only
minimally) affect serum potassium levels. Additional
pharmacologic agents that induce potassium trans
port into the intracellular space include insulin,84,85
β2
‑receptor agonists84
and bicarbonate86
(Table 2).
However, the efficacy of intravenous bicarbonate for this
indication in patients on dialysis has been questioned.87,88
The effects of interventions that alter the distribution of
potassium usually occur within a short period of time
(1 h), but they do not affect total body potassium levels.
Definitive therapy for hyperkalaemia in patients with
a net positive potassium balance necessitates the removal
of potassium from the body. Removal can be achieved
through enhanced renal excretion (for example, forced
diuresis with loop diuretics), but this approach might not
be effective in patients with limited GFR, such as those
with advanced CKD and ESRD. Increasing gastrointes
tinal excretion of potassium, through the administra
tion of potassium-binding resins (sodium polystyrene
sulphonate or calcium polystyrene sulphonate), has been
widely used to control acute hyperkalaemia, not only in
patients with ESRD and CKD, but also in patients with
Table 2 | Interventions used for acute or chronic treatment of hyperkalaemia
Treatment Route of
administration
Onset of action,
duration of effect
Mechanism Comments
6.8 mmol of calcium,
corresponding to 10 ml
CaCl (10%)* or 30 ml
calcium gluconate (10%)
solutions
Intravenous (acute) 1–3 min
30–60 min
Membrane potential
stabilization
Does not affect serum potassium level
Effect measured by normalization of
electrocardiographic changes
Dose can be repeated if no effects noted
Caution advised in patients receiving
digoxin
50–250 ml hypertonic
saline (3–5%)‡76,77
Intravenous (acute) 5–10 min
~2 h
Membrane potential
stabilization
Efficacy only in hyponatraemic patients
50–100 mmol sodium
bicarbonate
Intravenous (acute)
or oral (chronic)
5–10 min
~2 h
Redistribution Efficacy questioned for acute treatment
of patients on dialysis
10 units of regular insulin Intravenous (acute) 30 min
4–6 h
Redistribution Administer with 50 g of glucose
intravenously to prevent hypoglycaemia
β2
‑receptor agonists:
10–20 mg aerosol
(nebulized) or 0.5 mg in
100 ml of 5% dextrose
in water (intravenous)
Intravenous or
nebulized (both
acute)
30 min
2–4 h
Redistribution Effect independent of insulin and
aldosterone
Caution in patients with known
coronary artery disease
40 mg furosemide or
equivalent dose of other
loop diuretic. Higher doses
may be needed in patients
with advanced CKD
Intravenous (acute)
or oral (chronic)
Varies
Until diuresis
present or longer1
Excretion Loop diuretics for acute intervention
Loop or thiazide diuretics for chronic
management
Fludrocortisone acetate
≥0.1 mg (up to 0.4–
1.0 mg daily)
Oral (chronic) NA Excretion In patients with aldosterone deficiency
Large doses might be needed to
effectively lower potassium levels
Sodium retention, oedema and
hypertension might occur
Cation exchange resins
25–50 g
Oral or rectal
(either acute or
chronic), with or
without sorbitol
1–2 h
≥4–6 h§
Excretion Sodium polystyrene sulphonate is the
only approved agent in most countries
Calcium polystyrene sulphonate
is approved in some countries
New agents are in development
Dialysis Haemodialysis
(acute or chronic);
peritoneal dialysis
(chronic)
Within minutes
Until end of
dialysis or longer§
Removal Effects of dialysis on serum sodium,
bicarbonate, calcium and/or
magnesium levels can affect results
*CaCl is caustic and could damage peripheral veins. ‡
Limited data available from clinical studies. §
Effects can last for an unspecified length of time depending
on ongoing potassium intake or cellular redistribution. Abbreviations: CKD, chronic kidney disease; NA, not applicable.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved
- 6. 6 | ADVANCE ONLINE PUBLICATION www.nature.com/nrneph
normal kidney function.72
The approval of sodium poly
styrene sulphonate for the treatment of hyperkalaemia
by the FDA was based on a clinical trial published in
1961, in which 32 hyperkalaemic patients with severe
azotaemia showed a decrease in serum potassium of
0.9 mmol/l in the first 24 h following the administration
of this drug.89
Subsequently, the addition of sorbitol to
sodium polystyrene sulphonate was advocated to allevi
ate the constipation associated with its use.90
In 2014,
a retrospective analysis of data from 154 hospitalized
patients with hyperkalaemia (mean serum potassium
level 5.9 mmol/l) showed that administration of sodium
polystyrene sulphonate resulted in dose-dependent
reductions in serum potassium of 0.7–1.1 mmol/l.72
Administration of the highest doses of sodium poly
styrene sulphonate was associated with the best response
in patients treated with this agent alone. However, con
comitant administration of other antihyperkalaemic
therapies was associated with a greater decrease in serum
potassium levels than was observed in patients receiving
sodium polystyrene sulphonate alone, although only a
few patients received combination treatment.72
Of note, dialysis was not yet available at the time when
sodium polystyrene sulphonate was initially introduced
and few or no alternative therapies could be offered to
hyperkalaemic patients, which perhaps contributed
to the widespread application of this treatment in clini
cal practice. However, the utility and safety of sodium
polystyrene sulphonate in the treatment of hyperkalae
mia is now being questioned. Serum potassium levels
typically do not decline until several hours after the
administration of oral sodium polystyrene sulphonate,91
which makes this agent inappropriate as an emergency
intervention and might delay the initiation of definitive
therapies. Furthermore, several researchers have ques
tioned the effectiveness of sodium polystyrene sulpho
nate in lowering serum potassium levels,92–94
and some
have suggested that the effects of cathartics, such as
sorbitol, mixed with the sodium polystyrene sulphonate
might in fact be responsible for most of the potassium-
lowering effect seen after its administration.93
In normo
kalaemic individuals, careful measurements of faecal
potassium excretion after the administration of sodium
polystyrene sulphonate combined with either a cathar
tic (sorbitol or phenolphthalein) or placebo indicated no
significant increase in gastrointestinal excretion of potas
sium attributable to the resin.95
This lack of effect might be
explained by the low potassium concentration gradients
in normokalaemic patients, but also by the fact that the
capacity of sodium polystyrene sulphonate to exchange
potassium for sodium is about 33%, such that only about
40 mmol of potassium can be bound and excreted by a
30 g dose of the drug.96
Questions about the effective
ness of potassium-binding resins are compounded by
concerns about their safety, with several case reports
describing severe upper and lower gastrointestinal inju
ries following administration of these drugs.97–100
A litera
ture review found 30 reports describing 58 patients with
a gastrointestinal injury following the administration of
sodium polystyrene sulphonate. Most were injuries to the
colon (of which 62% involved transmural necrosis) and
the mortality rate was 33%.101
Although case reports can
provide an important safety warning, only a few studies
have attempted to systematically assess the frequency
of complications associated with sodium polystyrene
sulphonate. In a retrospective study of 752 hospitalized
patients exposed to sodium polystyrene sulphonate in
sorbitol the incidence of colonic necrosis was 0.3% overall,
and all cases of this complication occurred in patients
who received this treatment within 1 week after under
going surgery (2 of 117 patients, 1.8%). By contrast, no
colonic necrosis was identified in 862 control patients
who had undergone haemodialysis or organ transplanta
tion but did not receive sodium polystyrene sulphonate.102
However, in a subsequent, retrospective cohort study of
123,391 hospitalized patients, of whom 2,194 received
sodium polystyrene sulphonate in sorbitol, episodes of
colonic necrosis occurred in 0.14% of patients receiving
sodium polystyrene sulphonate and 0.07% of those not
exposed to this drug.103
To date it remains unclear whether
gastrointestinal toxicity is a consequence of polystyrene
sulphonate alone or whether exacerbating factors need
to be present. Experimental studies suggest that the sorbi
tol added to sodium polystyrene sulphonate is the main
exacerbating factor for colonic necrosis.104
However, some
case reports suggest that polystyrene sulphonate deriva
tives administered without sorbitol can also cause gastro
intestinal toxicity.99,100
Owing to these safety concerns, the
FDA issued a black box warning in 2009, recommending
against mixing sodium polystyrene sulphonate with 70%
sorbitol.105
Nonetheless, utilization of this agent (with and
without sorbitol at a 33% concentration) for the acute
treatment of hyperkalaemia remains widespread.72
In summary, acute management of hyperkalaemia
involves various interventions, including the intravenous
administration of calcium salts or drugs that affect the
cellular distribution of potassium, and definitive meas
ures to remove potassium from the body. Haemodialysis
is an effective acute therapy, but it is invasive and requires
specialized equipment and personnel. Forced diuresis
could be an option in patients with adequate kidney
function, but data are lacking on its efficacy and safety.
In patients with impaired kidney function and when
acute dialysis is not available,106
potassium binding resins
remain the only therapeutic option. Sodium polystyrene
sulphonate (which is currently the only potassium-
binding resin approved for lowering of serum potassium
levels in most countries, although calcium polystyrene
sulphonate is also used in some places) is still consid
ered an effective treatment for acute hyperkalaemia.72
However, questions about its safety profile remain.
Chronic management
The chronic management of hyperkalaemia presents
a fundamentally different challenge compared to its
acute treatment. Contrary to acute potassium-lowering
interventions, which are intended to achieve immedi
ate restoration of the cell membrane’s normal electro
physiologic milieu to avert cardiac arrhythmias, chronic
management aims to prevent the development of
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved
- 7. NATURE REVIEWS | NEPHROLOGY ADVANCE ONLINE PUBLICATION | 7
hyperkalaemia by correcting the underlying defects in
potassium homeostasis.
Chronic management of hyperkalaemia usually starts
by identifying and eliminating correctable causes, such as
a high potassium intake, hyperkalaemia-inducing medi
cations or metabolic acidosis. Effective interventions
include dietary education and a review of prescribed,
over-the-counter and herbal medications. In addition,
kaliuretic diuretics and sodium bicarbonate can be
administered (Table 2).17
Administration of aldosterone
(in the form of oral fludrocortisone acetate) is effective
in patients with aldosterone deficiency,107
but high doses
might be needed, which can induce sodium retention,
oedema and hypertension.
Unfortunately, some of the most strong hyperkalaemia-
inducing medications are RAAS inhibitors, which are
administered to patients with CKD and other comorbidi
ties because of their beneficial effects on clinical outcomes,
as discussed earlier. However, in many patients, recurrent
and/or severe hyperkalaemia makes the use of these medi
cations impossible, depriving patients of their beneficial
effects. Although discontinuation of RAAS inhibitors
very often resolves hyperkalaemia in patients with CKD,
implementation of alternative measures that might enable
continuation of these medications would be desirable.
Dietary modifications, the addition of diuretics (which
could have the added benefit of improved blood pressure
control) and correction of metabolic acidosis could be
beneficial and could occasionally allow continuation of
the RAAS inhibitors.
Another potential solution could be the use of novel
nonsteroidal mineralocorticoid-receptor antagonists. A
phase II clinical trial examining one such agent (finer
enone) in patients with chronic heart failure indicated
a reduced incidence of hyperkalaemia compared with
spironolactone.108
A similar phase II trial of finerenone
(versus eplerenone) in patients with heart failure and
either diabetes or moderate to advanced CKD is cur
rently underway.109
Phase III clinical trials are awaited to
confirm these early promising findings.
Potassium binders
If the above interventions do not resolve hyperkalaemia,
the addition of potassium-binding resins might be neces
sary. However, the few studies that have evaluated the
efficacy of sodium polystyrene sulphonate for the treat
ment of hyperkalaemia were performed in patients with
acute hyperkalaemia,89,90
and very limited information is
available on the efficacy and safety of this agent for the
chronic management of hyperkalaemia. In a retrospec
tive study of 14 patients with RAAS-inhibitor-associated
hyperkalaemia who were treated with daily sorbitol-free
sodium polystyrene sulphonate, serum potassium levels
were adequately controlled and no patients developed
colonic necrosis.110
However, given the low frequency of
this complication, larger studies are needed to assess the
efficacy, and especially the safety, of sodium polystyrene
sulphonate in this setting.
Potassium-binding medications other than sodium
polystyrene sulphonate could soon become available.
These new agents will have to undergo rigorous clini
cal trials before they can be approved for clinical use.
Hence, clinicians will hopefully have more certainty
than is possible for sodium polystyrene sulphonate about
their expected benefits and risks. Two new agents are
currently in advanced stages of clinical development for
the management of chronic hyperkalaemia. Patiromer is
an oral, non-absorbed, high-capacity potassium binder.
In a placebo-controlled trial involving 120 patients
with heart failure who had discontinued RAAS inhibi
tors because of hyperkalaemia and were starting treat
ment with an aldosterone antagonist, the patients who
received patiromer experienced serum potassium levels
that were 0.45 mmol/l lower than those in patients who
received placebo. The incidence of hyperkalaemia was
also lower in the patiromer group than in the placebo
group (7.3% versus 24.5%, respectively), and more
patients in the active drug group than in the placebo
group were able to tolerate spironolactone at a daily dose
of 50 mg.111,112
Another new agent is ZS‑9, which is a highly selective,
oral sorbent designed to preferentially trap potassium
ions throughout the gastrointestinal tract. In vitro studies
showed that ZS‑9 has a potassium-binding capacity of
≤3.5 mmol/g, exceeding the capacity of existing polymer-
based resins.113
ZS‑9 consists of an inorganic crystal, zir
conium silicate, rather than an organic polymer resin,
which could be important for differentiating its effects
from those of nonselective ion binders. The clinical
development of this agent includes assessments of its
role in the treatment of acute and chronic hyperkalaemia,
regardless of the underlying cause. Publication of results
from clinical trials assessing the efficacy and safety of
ZS‑9 is pending.
The use of potassium binders might be a realistic pos
sibility for the treatment of patients with chronic hyper
kalaemia, but dedicated studies are required to prove a
benefit over current practices.
Haemodialysis
Finally, chronic maintenance dialysis remains the princi
pal means to control potassium balance in patients with
ESRD, especially those without residual kidney function.
The current treatment paradigms for patients receiving
routine haemodialysis are, however, potentially hazard
ous for patients prone to hyperkalaemia. To avoid the
accumulation of potassium in patients with a normal or
high potassium intake, low-potassium dialysates must
be used. This approach achieves a net even potassium
balance, but results in marked fluctuations in serum
potassium levels: they gradually rise to high predialy
sis levels, only to fall to much lower levels in a short
period of time during and after dialysis. Such very rapid
changes in extracellular potassium concentration could
be hazardously arrhythmogenic. Although formal clini
cal trials are lacking, the available observational studies
suggest that predialysis hyperkalaemia is associated
with increased mortality4
and that use of low-potassium
dialysates is associated with an increased risk of sudden
cardiac death.63
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved
- 8. 8 | ADVANCE ONLINE PUBLICATION www.nature.com/nrneph
Potential solutions for this problem include extending
the duration of dialysis, which could enable the use of
dialysates with higher potassium concentrations, increas
ing the frequency of dialysis sessions, or prescribing
potassium binders (as discussed above) to patients on
chronic dialysis. Alternative dialysis strategies could have
additional benefits besides enabling more physiologic
potassium homeostasis, but their widespread applica
tion is hampered by financial and other considerations,
such as inconvenience to patients, insufficient capacity
for large-scale daily inpatient dialysis or the inability of
many patients to perform home-based dialysis.
Another obstacle to chronic management of hyper
kalaemia in patients on dialysis is infrequent monitor
ing of serum potassium levels, which are typically only
measured once a month. Fluctuations in serum potas
sium could occur on a daily basis as a result of dietary
changes or other factors (for example, intermittent
diarrhoea), which might necessitate adjustment of the
dialysate potassium concentration. Such fluctuations
in serum potassium are currently not detected, and
many patients on chronic haemodialysis might, there
fore, receive dialysis therapy using inappropriately low
or high dialysate potassium concentrations. The extent
and the clinical importance of this problem are unknown
because no published studies have assessed the frequency
and magnitude of fluctuations in serum potassium level
in individuals receiving chronic haemodialysis in the
outpatient setting. In a large observational study, the use
of an inappropriate dialysate potassium concentration
(relative to serum potassium concentration) was associ
ated with increased mortality.4
However, this study only
required the assessment of participants’ serum potassium
levels once a month and was not designed to provide
in-depth information about this problem.
Conclusions
Hyperkalaemia is common in patients with CKD, in
part because of their impaired kidney function and
in part because of the medications used to treat CKD
and the many ancillary effects of various comorbid con
ditions that can occur in this population of patients.
Both the acute and chronic management of hyperkalae
mia are important, owing to the severe arrhythmias that
can potentially be caused by hyperkalaemia. The most
vexing clinical problem is the management of hyper
kalaemia in patients receiving RAAS inhibitors, as the
known beneficial effects of these agents on both kidney
function and cardiovascular disease make their discon
tinuation undesirable. Nonetheless, discontinuation
rates of these agents remain very high in patients with
CKD.30
The development of new potassium-lowering
medications—more than 50 years after the approval of
sodium polystyrene sulphonate—might lead to renewed
efforts towards improved hyperkalaemia management. A
therapeutic paradigm shift from intermittent manage
ment of incidentally discovered acute hyperkalaemia
towards preventive measures aimed at normalizing
potassium homeostasis and thereby preventing large
fluctuations in serum potassium levels could prove
beneficial both by avoiding hyperkalaemic episodes
and by enabling the continued use of beneficial (but
hyperkalaemia-inducing) medications.
Review criteria
Full-text articles written in English and published between
1955 and March 2014 were identified using the PubMed
database. The following search terms were used:
“potassium”, “chronic kidney disease”, “hyperkalaemia”,
“outcomes”, “mortality” and “treatment”.
1. Lowrie, E. G. Lew, N. L. Death risk in
hemodialysis patients: the predictive value of
commonly measured variables and an evaluation
of death rate differences between facilities. Am.
J. Kidney Dis. 15, 458–482 (1990).
2. Iseki, K. et al. Impact of the initial levels of
laboratory variables on survival in chronic dialysis
patients. Am. J. Kidney Dis. 28, 541–548 (1996).
3. Hayes, J. et al. Association of hypo- and
hyperkalemia with disease progression and
mortality in males with chronic kidney disease:
the role of race. Nephron Clin. Pract. 120,
c8–c16 (2012).
4. Kovesdy, C. P. et al. Serum and dialysate
potassium concentrations and survival in
hemodialysis patients. Clin. J.Am. Soc. Nephrol.
2, 999–1007 (2007).
5. Gonick, H. C., Kleeman, C. R., Rubini, M. E.
Maxwell, M. H. Functional impairment in chronic
renal disease. III. Studies of potassium
excretion. Am. J. Med. Sci. 261, 281–290 (1971).
6. Hayes, C. P. Jr Robinson, R. R. Fecal
potassium excretion in patients on chronic
intermittent hemodialysis. Trans.Am. Soc.Artif.
Intern. Organs 11, 242–246 (1965).
7. Hayes, C. P. Jr, McLeod, M. E. Robinson, R. R.
An extrarenal mechanism for the maintenance
of potassium balance in severe chronic renal
failure. Trans.Assoc.Am. Physicians 80, 207–216
(1967).
8. Kopple, J. D. Coburn, J. W. Metabolic studies
of low protein diets in uremia. I. Nitrogen and
potassium. Medicine (Baltimore) 52, 583–595
(1973).
9. Schrier, R. W. Regal, E. M. Influence of
aldosterone on sodium, water and potassium
metabolism in chronic renal disease. Kidney Int.
1, 156–168 (1972).
10. Bourgoignie, J. J., Kaplan, M., Pincus, J.,
Gavellas, G. Rabinovitch, A. Renal handling
of potassium in dogs with chronic renal
insufficiency. Kidney Int. 20, 482–490 (1981).
11. Simmons, D. H. Avedon, M. Acid-base
alterations and plasma potassium concentration.
Am. J. Physiol. 197, 319–326 (1959).
12. Adrogué, H. J. Madias, N. E. Changes in plasma
potassium concentration during acute acid-base
disturbances. Am. J. Med. 71, 456–467 (1981).
13. Graber, M. A model of the hyperkalemia
produced by metabolic acidosis. Am. J. Kidney
Dis. 22, 436–444 (1993).
14. Magner, P. O., Robinson, L., Halperin, R. M.,
Zettle, R. Halperin, M. L. The plasma
potassium concentration in metabolic acidosis:
a re-evaluation. Am. J. Kidney Dis. 11, 220–224
(1988).
15. Oster, J. R., Perez, G. O. Vaamonde, C. A.
Relationship between blood pH and potassium
and phosphorus during acute metabolic acidosis.
Am. J. Physiol. 235, F345–F351 (1978).
16. Michael, J. M., Dorner, I., Bruns, D.,
Ladenson, J. H. Sherman, L. A. Potassium
load in CPD-preserved whole blood and two
types of packed red blood cells. Transfusion 15,
144–149 (1975).
17. Palmer, B. F. Managing hyperkalemia caused by
inhibitors of the renin‑angiotensin‑aldosterone
system. N. Engl. J. Med. 351, 585–592 (2004).
18. Heering, P. J. et al. Aldosterone resistance in
kidney transplantation is in part induced by a
down-regulation of mineralocorticoid receptor
expression. Clin.Transplant. 18, 186–192
(2004).
19. Laine, J. Holmberg, C. Renal and adrenal
mechanisms in cyclosporine-induced
hyperkalaemia after renal transplantation. Eur. J.
Clin. Invest. 25, 670–676 (1995).
20. DeFronzo, R. A., Sherwin, R. S., Felig, P. Bia, M.
Nonuremic diabetic hyperkalemia. Possible role
of insulin deficiency. Arch. Intern. Med. 137,
842–843 (1977).
21. Glassock, R. J., Goldstein, D. A., Goldstone, R.
Hsueh, W. A. Diabetes mellitus, moderate renal
insufficiency and hyperkalemia. Am. J. Nephrol.
3, 233–240 (1983).
22. Tuck, M. L., Sambhi, M. P. Levin, L.
Hyporeninemic hypoaldosteronism in diabetes
mellitus. Studies of the autonomic nervous
system’s control of renin release. Diabetes 28,
237–241 (1979).
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved
- 9. NATURE REVIEWS | NEPHROLOGY ADVANCE ONLINE PUBLICATION | 9
23. Arrizabalaga, P. et al. Increase in serum
potassium caused by β‑2 adrenergic blockade in
terminal renal failure: absence of mediation by
insulin or aldosterone. Proc. Eur. Dial.Transplant
Assoc. 20, 572–576 (1983).
24. Edes, T. E. Sunderrajan, E. V. Heparin-induced
hyperkalemia. Arch. Intern. Med. 145,
1070–1072 (1985).
25. Bismuth, C., Gaultier, M., Conso, F.
Efthymiou, M. L. Hyperkalemia in acute digitalis
poisoning: prognostic significance and
therapeutic implications. Clin.Toxicol. 6,
153–162 (1973).
26. Bühler, F. R. et al. Antihypertensive β blocking
action as related to renin and age: a
pharmacologic tool to identify pathogenetic
mechanisms in essential hypertension. Am. J.
Cardiol. 36, 653–669 (1975).
27. Pedersen, E. B. Kornerup, H. J. Relationship
between plasma aldosterone concentration and
plasma potassium in patients with essential
hypertension during alprenolol treatment. Acta
Med. Scand. 200, 263–267 (1976).
28. Bakris, G. L. et al. ACE inhibition or angiotensin
receptor blockade: impact on potassium in renal
failure. VAL‑K Study Group. Kidney Int. 58,
2084–2092 (2000).
29. Weir, M. R. Rolfe, M. Potassium homeostasis
and renin‑angiotensin‑aldosterone system
inhibitors. Clin. J.Am. Soc. Nephrol. 5, 531–548
(2010).
30. Molnar, M. Z. et al. Angiotensin-converting enzyme
inhibitor and angiotensin receptor blocker use
and mortality in patients with chronic kidney
disease. J.Am. Coll. Cardiol. 63, 650–658 (2014).
31. Pun, P. H., Lehrich, R. W., Smith, S. R.
Middleton, J. P. Predictors of survival after
cardiac arrest in outpatient hemodialysis clinics.
Clin. J.Am. Soc. Nephrol. 2, 491–500 (2007).
32. Fleet, J. L. et al. Validity of the International
Classification of Diseases 10th
revision code
for hyperkalaemia in elderly patients at
presentation to an emergency department and
at hospital admission. BMJ Open 2, e002011
(2012).
33. Einhorn, L. M. et al. The frequency of
hyperkalemia and its significance in chronic
kidney disease. Arch. Intern. Med. 169,
1156–1162 (2009).
34. Drawz, P. E., Babineau, D. C. Rahman, M.
Metabolic complications in elderly adults with
chronic kidney disease. J.Am. Geriatr. Soc. 60,
310–315 (2012).
35. Sarafidis, P. A. et al. Prevalence and factors
associated with hyperkalemia in predialysis
patients followed in a low-clearance clinic. Clin. J.
Am. Soc. Nephrol. 7, 1234–1241 (2012).
36. Makani, H., Bangalore, S., Desouza, K. A.,
Shah, A. Messerli, F. H. Efficacy and safety of
dual blockade of the renin–angiotensin system:
meta-analysis of randomised trials. BMJ 346,
f360 (2013).
37. Susantitaphong, P. et al. Efficacy and safety
of combined vs. single renin‑angiotensin‑
aldosterone system blockade in chronic kidney
disease: a meta-analysis. Am. J. Hypertens. 26,
424–441 (2013).
38. Lewis, E. J., Hunsicker, L. G., Bain, R. P.
Rohde, R. D. The effect of angiotensin‑
converting‑enzyme inhibition on diabetic
nephropathy. The Collaborative Study Group.
N. Engl. J. Med. 329, 1456–1462 (1993).
39. Maschio, G. et al. Effect of the
angiotensin‑converting‑enzyme inhibitor
benazepril on the progression of chronic renal
insufficiency. The Angiotensin‑Converting‑Enzyme
Inhibition in Progressive Renal Insufficiency Study
Group. N. Engl. J. Med. 334, 939–945 (1996).
40. [No authors listed] Randomised placebo-
controlled trial of effect of ramipril on decline
in glomerular filtration rate and risk of terminal
renal failure in proteinuric, non-diabetic
nephropathy. The GISEN Group (Gruppo Italiano
di Studi Epidemiologici in Nefrologia). Lancet
349, 1857–1863 (1997).
41. Ruggenenti, P. et al. Blood-pressure control for
renoprotection in patients with non-diabetic
chronic renal disease (REIN‑2): multicentre,
randomised controlled trial. Lancet 365,
939–946 (2005).
42. Mann, J. F., Gerstein, H. C., Pogue, J., Bosch, J.
Yusuf, S. Renal insufficiency as a predictor
of cardiovascular outcomes and the impact of
ramipril: the HOPE randomized trial. Ann. Intern.
Med. 134, 629–636 (2001).
43. Weinberg, J. M. et al. Risk of hyperkalemia in
nondiabetic patients with chronic kidney disease
receiving antihypertensive therapy. Arch. Intern.
Med. 169, 1587–1594 (2009).
44. Iino, Y. et al. Renoprotective effect of losartan
in comparison to amlodipine in patients with
chronic kidney disease and hypertension
—a report of the Japanese Losartan Therapy
Intended for the Global Renal Protection in
Hypertensive Patients (JLIGHT) study. Hypertens.
Res. 27, 21–30 (2004).
45. Miao, Y. et al. Increased serum potassium
affects renal outcomes: a post hoc analysis of
the Reduction of Endpoints in NIDDM with the
Angiotensin II Antagonist Losartan (RENAAL)
trial. Diabetologia 54, 44–50 (2011).
46. Fried, L. F. et al. Combined angiotensin inhibition
for the treatment of diabetic nephropathy.
N. Engl. J Med. 369, 1892–1903 (2013).
47. Sanofi Aventis US. Avapro©
package insert
[online], http://products.sanofi.us/Avapro/
Avapro.pdf (2014).
48. Hou, F. F. et al. Efficacy and safety of benazepril
for advanced chronic renal insufficiency. N. Engl.
J. Med. 354, 131–140 (2006).
49. Bozkurt, B., Agoston, I. Knowlton, A. A.
Complications of inappropriate use of
spironolactone in heart failure: when an old
medicine spirals out of new guidelines. J.Am.
Coll. Cardiol. 41, 211–214 (2003).
50. Shah, K. B., Rao, K., Sawyer, R. Gottlieb, S. S.
The adequacy of laboratory monitoring in
patients treated with spironolactone for
congestive heart failure. J.Am. Coll. Cardiol. 46,
845–849 (2005).
51. Juurlink, D. N. et al. Rates of hyperkalemia
after publication of the Randomized Aldactone
Evaluation Study. N. Engl. J. Med. 351, 543–551
(2004).
52. Knoll, G. A. et al. Renin–angiotensin system
blockade and the risk of hyperkalemia in
chronic hemodialysis patients. Am. J. Med. 112,
110–114 (2002).
53. Ito, Y. et al. Long-Term effects of spironolactone
in peritoneal dialysis patients. J.Am. Soc.
Nephrol. 25, 1094–1102 (2014).
54. Vazquez-Rangel, A. et al. Spironolactone to
prevent peritoneal fibrosis in peritoneal dialysis
patients: a randomized controlled trial. Am. J.
Kidney Dis. 63, 1072–1074 (2014).
55. Matsumoto, Y. et al. Spironolactone reduces
cardiovascular and cerebrovascular morbidity
and mortality in hemodialysis patients. J.Am.
Coll. Cardiol. 63, 528–536 (2014).
56. Flevari, P. et al. Spironolactone improves
endothelial and cardiac autonomic function
in non heart failure hemodialysis patients.
J. Hypertens. 31, 1239–1244 (2013).
57. Shavit, L., Neykin, D., Lifschitz, M. Slotki, I.
Effect of eplerenone on blood pressure and
the renin‑angiotensin‑aldosterone system in
oligo-anuric chronic hemodialysis patients
—a pilot study. Clin. Nephrol. 76, 388–395
(2011).
58. Vukusich, A. et al. A randomized, double-blind,
placebo-controlled trial of spironolactone on
carotid intima–media thickness in nondiabetic
hemodialysis patients. Clin. J.Am. Soc. Nephrol.
5, 1380–1387 (2010).
59. Hammer, F. et al. Rationale and design of the
Mineralocorticoid Receptor Antagonists in End-
Stage Renal Disease Study (MiREnDa). Nephrol.
Dial.Transplant. 29, 400–405 (2014).
60. Dittrich, K. L. Walls, R. M. Hyperkalemia: ECG
manifestations and clinical considerations.
J. Emerg. Med. 4, 449–455 (1986).
61. Parham, W. A., Mehdirad, A. A., Biermann, K. M.
Fredman, C. S. Hyperkalemia revisited. Tex.
Heart Inst. J. 33, 40–47 (2006).
62. Korgaonkar, S. et al. Serum potassium and
outcomes in CKD: insights from the RRI-CKD
cohort study. Clin. J.Am. Soc. Nephrol. 5,
762–769 (2010).
63. Pun, P. H., Lehrich, R. W., Honeycutt, E. F.,
Herzog, C. A. Middleton, J. P. Modifiable risk
factors associated with sudden cardiac arrest
within hemodialysis clinics. Kidney Int. 79,
218–227 (2011).
64. Jadoul, M. et al. Modifiable practices associated
with sudden death among hemodialysis patients
in the Dialysis Outcomes and Practice Patterns
Study. Clin. J.Am. Soc. Nephrol. 7, 765–774
(2012).
65. Xu, Q. et al. Serum potassium levels and its
variability in incident peritoneal dialysis patients:
associations with mortality. PLoS ONE 9,
e86750 (2014).
66. Epstein, F. H. Signs and symptoms of electrolyte
disorders. In Clinical disorders of fluid and
electrolyte metabolism (eds Maxwell, M. H.
Kleeman, C. R.) 499–516 (McGraw-Hill, 1980).
67. Fisch, C. Electrolytes and the heart. In The Heart
(ed. Hurst, J. W.) 1466–1479 (McGraw-Hill,
1986).
68. Kleeman, K. Singh, B. N. Serum electrolytes
and the heart. In Clinical disorders of fluid and
electrolyte metabolism (eds Maxwell, M. H.
Kleeman, C. R.) 145–180 (McGraw-Hill, 1980).
69. Marques, J. S. Diogo, A. N. Dead man walking:
an extreme case of sinusoidal wave pattern in
severe hyperkalemia. J.Am. Coll. Cardiol. 59,
2118 (2012).
70. Petrov, D. B. Images in clinical medicine. An
electrocardiographic sine wave in hyperkalemia.
N. Engl. J. Med. 366, 1824 (2012).
71. Siniorakis, E. et al. Hyperkalaemia,
pseudohyperkalaemia and electrocardiographic
correlates. Int. J. Cardiol. 148, 242–243 (2011).
72. Fordjour, K. N., Walton, T. Doran, J. J.
Management of hyperkalemia in hospitalized
patients. Am. J. Med. Sci. 347, 93–100 (2014).
73. Montague, B. T., Ouellette, J. R. Buller, G. K.
Retrospective review of the frequency of ECG
changes in hyperkalemia. Clin. J.Am. Soc.
Nephrol. 3, 324–330 (2008).
74. Green, D., Green, H. D., New, D. I. Kalra, P. A.
The clinical significance of hyperkalaemia-
associated repolarization abnormalities in end-
stage renal disease. Nephrol. Dial.Transplant.
28, 99–105 (2013).
75. Welch, A., Maroz, N. Wingo, C. S.
Hyperkalemia: getting to the heart of the matter.
Nephrol. Dial.Transplant. 28, 15–16 (2013).
76. Garcia-Palmieri, M. R. Reversal of hyperkalemic
cardiotoxicity with hypertonic saline. Am. Heart. J.
64, 483–488 (1962).
77. Weisberg, L. S. Management of severe
hyperkalemia. Crit. Care Med. 36, 3246–3251
(2008).
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved
- 10. 10 | ADVANCE ONLINE PUBLICATION www.nature.com/nrneph
78. Beeler, G. W. Jr Reuter, H. Membrane calcium
current in ventricular myocardial fibres. J. Physiol.
207, 191–209 (1970).
79. Chen, C. M., Gettes, L. S. Katzung, B. G.
Effect of lidocaine and quinidine on steady-state
characteristics and recovery kinetics of (dV/dt)max
in guinea pig ventricular myocardium. Circ. Res.
37, 20–29 (1975).
80. Winkler, A. W., Hoff, H. E. Smith, P. K. Factors
affecting the toxicity of potassium. Am. J. Physiol.
127, 430–436 (1939).
81. Eliakim, M., Rosenberg, S. Z. Braun, K.
Electrocardiographic changes following the
administration of hypertonic saline to dogs.
Am. Heart J. 58, 97–101 (1959).
82. Kaplan, J. L. et al. Hypertonic saline treatment
of severe hyperkalemia in nonnephrectomized
dogs. Acad. Emerg. Med. 7, 965–973 (2000).
83. Ballantyne, F. 3rd
, Davis, L. D. Reynolds, E. W. Jr.
Cellular basis for reversal of hyperkalemic
electrocardiographic changes by sodium. Am. J.
Physiol. 229, 935–940 (1975).
84. Lens, X. M., Montoliu, J., Cases, A.,
Campistol, J. M. Revert, L. Treatment of
hyperkalaemia in renal failure: salbutamol v.
insulin. Nephrol. Dial.Transplant 4, 228–232
(1989).
85. Alvestrand, A., Wahren, J., Smith, D.
DeFronzo, R. A. Insulin-mediated potassium
uptake is normal in uremic and healthy subjects.
Am. J. Physiol. 246, E174–E180 (1984).
86. Schwarz, K. C., Cohen, B. D., Lubash, G. D.
Rubin, A. L. Severe acidosis and
hyperpotassemia treated with sodium
bicarbonate infusion. Circulation 19, 215–220
(1959).
87. Allon, M. Shanklin, N. Effect of bicarbonate
administration on plasma potassium in dialysis
patients: interactions with insulin and albuterol.
Am. J. Kidney Dis. 28, 508–514 (1996).
88. Mahoney, B. A. et al. Emergency interventions
for hyperkalaemia. Cochrane Database of
Systematic Reviews, Issue 2. Art. No.:
CD003235. http://dx.doi.org/10.1002/
14651858.CD003235.pub2.
89. Scherr, L., Ogden, D. A., Mead, A. W., Spritz, N.
Rubin, A. L. Management of hyperkalemia with
a cation-exchange resin. N. Engl. J. Med. 264,
115–119 (1961).
90. Flinn, R. B., Merrill, J. P. Welzant, W. R.
Treatment of the oliguric patient with a new
sodium-exchange resin and sorbitol;
a preliminary report. N. Engl. J. Med. 264,
111–115 (1961).
91. Emmett, M. et al. Effect of three laxatives and
a cation exchange resin on fecal sodium and
potassium excretion. Gastroenterology 108,
752–760 (1995).
92. Kamel, K. S. Wei, C. Controversial issues in
the treatment of hyperkalaemia. Nephrol. Dial.
Transplant. 18, 2215–2218 (2003).
93. Kamel, K. S. Schreiber, M. Asking the question
again: are cation exchange resins effective for
the treatment of hyperkalemia? Nephrol. Dial.
Transplant. 27, 4294–4297 (2012).
94. Sterns, R. H., Rojas, M., Bernstein, P.
Chennupati, S. Ion-exchange resins for the
treatment of hyperkalemia: are they safe and
effective? J.Am. Soc. Nephrol. 21, 733–735
(2010).
95. Gruy-Kapral, C. et al. Effect of single dose resin-
cathartic therapy on serum potassium
concentration in patients with end-stage renal
disease. J.Am. Soc. Nephrol. 9, 1924–1930
(1998).
96. Kayexalate®(sodium polystyrene sulfonate, USP
cation-exchange resin) FDA Drug Label [online],
http://www.accessdata.fda.gov/drugsatfda_
docs/label/2009/011287s021lbl.pdf (2009).
97. Chelcun, J. L., Sable, R. A. Friedman, K.
Colonic ulceration in a patient with renal disease
and hyperkalemia. JAAPA 25, 34, 37–38 (2012).
98. Gorospe, E. C., Lewis, J. T. Bruining, D. H.
Kayexalate-induced esophageal ulcer in a
patient with gastroparesis. Clin. Gastroenterol.
Hepatol. 10, A28 (2012).
99. Joo, M., Bae, W. K., Kim, N. H. Han, S. R.
Colonic mucosal necrosis following
administration of calcium polystryrene sulfonate
(Kalimate) in a uremic patient. J. Korean Med.
Sci. 24, 1207–1211 (2009).
100. Takeuchi, N. et al. Development of colonic
perforation during calcium polystyrene sulfonate
administration: a case report. Case Rep. Med.
2013, 102614 (2013).
101. Harel, Z. et al. Gastrointestinal adverse events
with sodium polystyrene sulfonate (Kayexalate)
use: a systematic review. Am. J. Med. 126,
264.e9–264.e24 (2013).
102. Gerstman, B. B., Kirkman, R. Platt, R. Intestinal
necrosis associated with postoperative orally
administered sodium polystyrene sulfonate in
sorbitol. Am. J. Kidney Dis. 20, 159–161 (1992).
103. Watson, M. A. et al. Association of prescription
of oral sodium polystyrene sulfonate with
sorbitol in an inpatient setting with colonic
necrosis: a retrospective cohort study. Am. J.
Kidney Dis. 60, 409–416 (2012).
104. Lillemoe, K. D. et al. Intestinal necrosis due to
sodium polystyrene (Kayexalate) in sorbitol
enemas: clinical and experimental support for
the hypothesis. Surgery 101, 267–272 (1987).
105. US Food and Drug Administration. Kayexalate
(sodium polystyrene sulfonate) powder. Safety
labeling changes approved by FDA Center for
Drug Evaluation and Research (CDER) [online],
http://www.fda.gov/Safety/MedWatch/
SafetyInformation/ucm186845.htm (2009).
106. Watson, M., Abbott, K. C. Yuan, C. M. Damned
if you do, damned if you don’t: potassium
binding resins in hyperkalemia. Clin. J. Am. Soc.
Nephrol. 5, 1723–1726 (2010).
107. DeFronzo, R. A. Hyperkalemia and hyporeninemic
hypoaldosteronism. Kidney Int. 17, 118–134
(1980).
108. Pitt, B. et al. Safety and tolerability of the novel
non-steroidal mineralocorticoid receptor
antagonist BAY 94–8862 in patients with chronic
heart failure and mild or moderate chronic
kidney disease: a randomized, double-blind trial.
Eur. Heart J. 34, 2453–2463 (2013).
109. US National Library of Medicine. ClinicalTrials.gov
[online], http://clinicaltrials.gov/show/
NCT01807221 (2014).
110. Chernin, G. et al. Secondary prevention of
hyperkalemia with sodium polystyrene
sulfonate in cardiac and kidney patients on
renin‑angiotensin‑aldosterone system inhibition
therapy. Clin. Cardiol. 35, 32–36 (2012).
111. Pitt, B. et al. Evaluation of the efficacy and safety
of RLY5016, a polymeric potassium binder, in a
double-blind, placebo-controlled study in
patients with chronic heart failure (the
PEARL-HF) trial. Eur. Heart J. 32, 820–828
(2011).
112. Buysse, J. M., Huang, I. Z. Pitt, B. PEARL-HF:
prevention of hyperkalemia in patients with heart
failure using a novel polymeric potassium binder,
RLY5016. Future Cardiol. 8, 17–28 (2012).
113. Yang, A., Leon, A., Nuttall, M., Low, J. J.,
Rasmussen, H. S. In vitro ion exchange capacity
and selectivity of ZS‑9, a novel, selective cation
trap for the treatment of hyperkalemia. Am. J.
Kidney Dis. 63, B115 (2014).
Acknowledgements
C.P.K. is supported by grants RO1 DK096920 and
UO1DK102163 from the US NIH-NIDDK. He is an
employee of the US Department of Veterans Affairs.
Opinions expressed in this paper are those of the
author and do not necessarily represent those of
the Department of Veterans Affairs.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved