Minarcik robbins 2013_ch19-pancreas
•Download as PPT, PDF•
1 like•732 views

This document provides an overview of the pancreas, including its embryology, anatomy, functions, blood supply, lymphatic drainage, and major diseases. It discusses the etiology and risk factors for pancreatic inflammation and neoplasms. Acute and chronic pancreatitis are covered in detail, including their causes, clinical features, morphology, and consequences. The document also summarizes pancreatic cysts and neoplasms such as serous cystadenoma, mucinous cystadenoma, intraductal papillary mucinous neoplasm, and pancreatic adenocarcinoma.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Minarcik robbins 2013_ch19-pancreas
Similar to Minarcik robbins 2013_ch19-pancreas (20)
More from Elsa von Licy
More from Elsa von Licy (20)
Recently uploaded
Recently uploaded (20)
Minarcik robbins 2013_ch19-pancreas
- 1. PANCREAS
- 3. OBJECTIVES • Understand the etiology/risk factors, pathogenesis, morphology, clinical features and outcome of pancreatic inflammations and neoplasms
- 5. Ventral Bud
- 9. Chapter 19
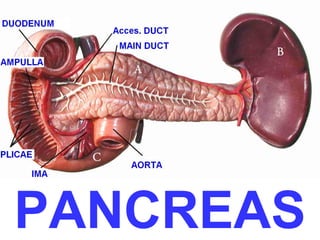
- 10. Posterior view of duodenum/pancreas
- 11. Arterial supply and venous drainage of the pancreas and spleen
- 12. Lymphatic drainage of the distal pancreas and spleen
- 14. Hepaticopancreatic ampulla (Ampulla of Vater)
- 15. L2
- 18. makes HCO3¯
- 22. PANCREAS DISEASES • Congenital • Inflammatory –Acute –Chronic • Cysts • Neoplasms
- 23. Congenital • Agenesis (very rare) • Pancreas Divisum (failure of 2 ducts to fuse) (common) • Annular Pancreas (pancreas encircles duodenum) (rare) • Ectopic Pancreas (very common)
- 26. PANCREATITIS • ACUTE (VERY SERIOUS) • CHRONIC (Calcifications, Pseudocyst)
- 27. CONSEQUENCES of ACUTE and CHRONIC pancreatitis
- 28. ACUTE PANCREATITIS • ALCOHOLISM • Bile reflux • • • • • • Medications (thiazides) Hypertriglyceridemia, hypercalcemia Acute ischemia Trauma, blunt, iatrogenic Genes: PRSS1, SPINK1 Idiopathic, 10-20%
- 29. CLINICAL FEATURES • ABDOMINAL PAIN • EXTREME emergency situation • HIGH mortality • …but MOST important lab test is……….?????
- 30. AMYLASE !!!!!!!
- 31. • • • • • • MORPHOLOGY EDEMA FAT NECROSIS ACUTE INFLAMMATORY INFILTRATE PANCREAS AUTODIGESTION BLOOD VESSEL DESTRUCTION “SAPONIFICATION” (stearates, Na+, Ca++)
- 34. CHRONIC PANCREATITIS • Pancreatic duct obstruction, LONGSTANDING • Tropical • Hereditary (PRSS1, SPINK1 mutations) • IDIOPATHIC (40%)
- 38. CLINICAL FEATURES • Abdominal Pain • Vague abdominal symptoms • Nothing • CT calcifications (why?), amylase elevated, chronic diarrhea if chronic pancreatic insuffiency develops, high likelihood of pseudocysts
- 39. PDEUDOCYSTS • Why “pseudo”? • STRONGLY linked with pancreatitis • Can be as big as a football and often are. • Can cause obstruction • Can get infected • Do NOT become malignant
- 42. Pancreas Neoplasms • • • • • • • Serous Mucinous Cystic Microcystic Papillary Benign Malignant (dense sclerosis is the rule)
- 47. Pancreatic CA
- 49. • • • • FATE: Regional lymph nodes Liver Often L-2 spine Lungs Grading (WMP), Staging, TNM
- 50. Final TIP of the day • Painless jaundice in an elderly person is CARCINOMA of the head of the pancreas until proven otherwise
Editor's Notes
- Perhaps the only thing that’s complicated about the pancreas, is its intimate relationship with the duodenum.
- The pancreas is the point in this course when I can start to see the light at the end of the tunnel!
- Know fates of dorsal and ventral buds.
- Know fates of dorsal and ventral buds.
- Know fates of dorsal and ventral buds.
- Know fates of dorsal and ventral buds. Now you know why the pancreas has TWO ducts!
- Know fates of dorsal and ventral buds.
- Know main anatomical landmarks and relationships to other organs
- Recall blood flow, arterial HEAD: Superior pancreatcoduodenal (A&P) arteries, from the gastroduodenal of the common hepatic of the CELIAC HEAD: Inferior pancreaticoduodenal (A&P) arteries from the SMA BODY and TAIL: SPLENIC
- “Peri-”pancreatic lymph nodes, several groups.
- Pancreatic duct, the MAIN one from the VENTRAL bud, “usually” empties into the most distal portion of the CBD (Common Bile Duct)
- EGD (Esophago, Gastro, Duodenoscopy) This is where a GI doc might be able to remove a lodges stone, or biopsy an ampullary tumor.
- Axial diagram.
- Typical CT landmarks.
- Typical CT landmarks, with contrast.
- Histology concepts. Centroacinarintercalatedintralobularinterlobular
- H&E, e.m.
- Histology, H&E Find an intercalated duct.
- Classical classification again, our old friend.
- Pancreas Divisum is failure of fusion of dorsal and ventral buds.
- Why is the pancreas known as the most “autolytic” of all organs? What does autolytic mean? What happens if you wait a few days before doing an autopsy?
- Does this look like a partly digested piece of meat? It is.
- Why the blurr? Microscope out of focus. What is autolysis?
- Chronic pancreatitis goes hand in hand with chronic alcoholism.
- Find the “soap”, find the calcium.
- Unfortunately dense fibrosis is a feature BOTH of chronic pancreatitis as well as adenocarcinoma, but in pancreatitis, the fibrotic acini are usually still following a lobular pattern)
- What is every pathologist’s nightmare? Ans: Getting a small needle biopsy of sclerosing pancreatitis and calling it it cancer on frozen section, getting the “Whipple” specimen the next day, and realizing you were WRONG! The patient has now undergone an operation which has a 10% mortality rate, for no reason, and the malpractice attorneys are at your door like jackals.
- Do you remember the anatomic area called the lesser sac?, also known as the omental bursa?
- Small pseudocyst, showing organizing inflamation on right
- Football sized pseudocyst, pretty much representing the entire lesser sac.
- These are also called “micro”-cystic, especially if the cysts are only easily recognized on microscopy.
- Various genetic alterations in the pathogenesis of pancreatic carcinoma. What to take home? Telomere shortening K-RAS mutations P16 inactivation Further inactivation of p53, SMAD4, BRCA2 More or less, in that order! This is a beautiful diagram because it correlates microscopic dysplastic changes with genetic alterations!
- Describe this in plain English.
- Gross fibrosis on left, microscopic on right.
- Perhaps “biologic behavior” is a better word than “fate”?