Minarcik robbins 2013_ch5-genetics
•Télécharger en tant que PPT, PDF•
1 j'aime•1,293 vues


Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Minarcik robbins 2013_ch5-genetics
Similaire à Minarcik robbins 2013_ch5-genetics (20)
Plus de Elsa von Licy
Plus de Elsa von Licy (20)
Dernier
Dernier (20)
Minarcik robbins 2013_ch5-genetics
- 3. MUTATIONS • PERMANENT change in DNA • GENE MUTATION: (may, and often, result in a single base error) • CHROMOSOME MUTATION: (visible chromosome change) • GENOME MUTATION: (whole chromosome)
- 4. GENE MUTATION • DELETION OF A SINGLE BASE • SUBSTITUTION OF A SINGLE BASE
- 6. GENE MUTATION • POINT MUTATION within a coding sequence: VAL-GLU • MUTATIONS in NON-coding sequences defective transcription, regulation • DELETIONS/INSERTIONS “frameshift” mutation, involvement is NOT a multiple of 3 • Tri-nucleotide REPEATS, e.g., CGG repeats many times in fragile X syndrome, CAG in others
- 7. GENE MUTATIONS • • • • • INTERFERE with protein synthesis SUPPRESS transcription, DNARNA PRODUCE abnormal mRNA DEFECTS carried over into TRANSLATION ABNORMAL proteins WITHOUT impairing syntheses
- 8. GENETIC DISORDERS • SINGLE gene mutations, following classical MENDELIAN inheritance patterns the most • MULTIFACTORIAL inheritance • CHROMOSOMAL disorders • NON-MENDELIAN disorders
- 9. MENDELIAN inheritance patterns • AUTOSOMAL DOMINANT • AUTOSOMAL RECESSIVE • SEX-LINKED (recessive), involving “X” chromosome
- 10. AUTOSOMAL DOMINANT • Disease is in HETEROZYGOTES • NEITHER parent may have the disease (NEW mut.) • REDUCED PENETRANCE (environment?, other genes?) • VARIABLE EXPRESSIVITY (environment?, other genes?) • May have a DELAYED ONSET • Usually result in a REDUCED PRODUCTION or INACTIVE protein
- 11. AUTOSOMAL DOMINANT • • • • • • • HUNTINGTON DISEASE NEUROFIBROMATOSIS MYOTONIC DYSTROPHY TUBEROUS SCLEROSIS POLYCYSTIC KIDNEY HEREDITARY SPHEROCYTOSIS VON WILLEBRAND DISEASE • • • • • • MARFAN SYNDROME EHLERS-DANLOS SYNDROMES (some) OSTEOGENESIS IMPERFECTA ACHONDROPLASIA FAMILIAL HYPERCHOLESTEROLEMIA ACUTE INTERMITTENT PORPHYRIA
- 12. AUTOSOMAL DOMINANT PEDIGREE 1) BOTH SEXES INVOLVED 2) GENERATIONS NOT SKIPPED
- 13. AUTOSOMAL RECESSIVE • Disease is in HOMOZYGOTES • More UNIFORM expression than AD • Often COMPLETE PENETRANCE • Onset usually EARLY in life • NEW mutations rarely detected clinically • Proteins show LOSS of FUNCTION • Include ALL inborn errors of metabolism • MUCH more common that autosomal dominant
- 14. AUTOSOMAL RECESSIVE • • • • • • • • • CF PKU GALACTOSEMIA HOMOCYSTINURIA LYSOSOMAL STORAGE Α-1 ANTITRYPSIN WILSON DISEASE HEMOCHROMATOSIS GLYCOGEN STORAGE DISEASES Hgb S THALASSEMIAS CONG. ADRENAL HYPERPLASIA EHLERS-DANLOS (some) ALKAPTONURIA NEUROGENIC MUSC. ATROPHIES FRIEDREICH ATAXIA SPINAL MUSCULAR ATROPHY
- 15. AUTOSOMAL RECESSIVE PEDIGREE 1) BOTH SEXES INVOLVED 2) GENERATIONS SKIPPED
- 16. SEX (“X”) LINKED • • • • MALES ONLY HIS SONS are OK, right? ALL his DAUGHTERS are CARRIERS The “Y” chromosome is NOT homologous to the “X”, i.e., the concept of dominant/recessive has no meaning here • HETEROZYGOUS FEMALES have no phenotypic expression (carriers)….usually, this means autosomal “recessive”, right?
- 17. SEX (“X”) LINKED • • • • • • • • DUCHENNE MUSCULAR DYSTROPHY HEMOPHILIA , A and B G6PD DEFICIENCY AGAMMAGLOBULINEMIA WISKOTT-ALDRICH SYNDROME DIABETES INSIPIDUS LESCH-NYHAN SYNDROME FRAGILE-X SYNDROME
- 18. SEX LINKED PEDIGREE 1) MALES ONLY, sons of affected males are OK 2) GENERATION SKIPPING DOESN’T MATTER
- 19. SINGLE GENE DISORDERS • ENZYME DEFECT (Most of them, e.g., PKU) – Accumulation of substrate – Lack of product – Failure to inactivate a protein which causes damage • RECEPTOR/TRANSPORT PROTEIN DEFECT (Familial Hypercholesterolemia) • STRUCTURAL PROTEIN DEFECT (Marfan, Ehl-Dan) – Structure – Function – Quantity • ENZYME DEFECT WHICH INCREASES DRUG SUSCEPTIBILITY: G6PDPrimaquine
- 20. STRUCTURAL PROTEIN DEFECTS • Marfan Syndrome – Fibrillin-1 defect (not -2 or -3) – Tall, dislocated lens, aortic arch aneurysms, etc. – Abraham Lincoln?, Osama bin-Laden • Ehlers-Danlos Syndromes (AD, AR) – Multiple (6?) different types – Classical, Hypermob., Vasc., KyphoSc., ArthChal., Derm – Various collagen defects – Hyperelastic skin, hyperextensible joints
- 21. RECEPTOR PROTEIN DEFECTS • FAMILIAL HYPERCHOLESTEROLEMIA – LDL RECEPTOR defect – Cholesterol TRANSPORT across liver cell impaired – ergo, CHOLESTEROL BUILDUP IN BLOOD • “Scavenger System” for CHOL kicks in, i.e., MACROPHAGES • YOU NOW KNOW THE REST OF THE STORY • YOU NOW KNOW WHY MACROPHAGES are “FOAMY”
- 22. ENZYME DEFICIENCIES • BY FAR, THE LARGEST KNOWN CATEGORY – SUBSTRATE BUILDUP – PRODUCT LACK – SUBSTRATE could be HARMFUL • LYSOSOMAL STORAGE DISEASES comprise MOST of them
- 23. LYSOSOMAL STORAGE DISEASES • • • • • • GLYCOGEN STORAGE DISEASES SPHINGOLIPIDOSES (Gangliosides) SULFATIDOSES MUCOPOLYSACCHARIDOSES MUCOLIPIDOSES OTHER – Fucosidosis, Mannosidosis, Aspartylglycosaminuria – WOLMAN, Acid phosphate deficiency
- 24. GLYCOGEN STORAGE DISEASES • MANY TYPES (at least 13) • Type 2 (Pompe), von Gierke, McArdle, most studied and discussed, and referred to • Storage sites: Liver, Striated Muscle (Skel + Ht)
- 25. SPHINGOLIPIDOSES • MANY types, Tay-Sachs most often referred to – – – – – GANGLIOSIDES are ACCUMULATED Ashkenazi Jews (1/30 are carriers) CNS neurons a site of accumulation CHERRY RED spot in Macula Usually fatal by age 4
- 26. SULFATIDOSES • MANY types, but the metachromatic leukodystrophies (CNS), Krabbe, Fabry, Gaucher, and Niemann-Pick (A and B) are most commonly referred to • SULFATIDES, CEREBROSIDES, SPHINGOMYELIN are the accumulations
- 27. • • • • • • NIEMANN-PICK TYPES A, B, C SPHINGOMYELIN BUILDUP Sphingomyelinase (ASM), is the missing enzyme MASSIVE SPLENOMEGALY ALSO in ASHKANAZI JEWS OFTEN FATAL in EARLY LIFE, CNS, ORGANOMEGALY
- 28. GAUCHER DISEASE • GLUCOCEREBROSIDE BUILDUP • 99% are type I, NO CNS involvement • ALL MACROPHAGES, liv, spl, nodes, marrow
- 29. MUCOPOLYSACCHARIDOSES • HURLER/HUNTER, for I and II, respectively • DERMATAN sulfate, HEPARAN sulfate buildup, respectively – coarse facial features – clouding of the cornea – joint stiffness – mental retardation – URINARY EXCRETION of SULFATES COMMON
- 30. OTHER LYSOSOMAL STORAGE DIS. • • • • • FUCOSIDOSIS MANNOSIDOSIS ASPARTYLGLYCOSAMINURIA WOLMAN (CHOL., TRIGLYCERIDES) ACID PHOSPHATE DEFICIENCY (PHOS. ESTERS)
- 31. ALCAPTONURIA • • • • NOT a LYSOSOMAL ENZYME DISEASE FIRST ONE TO BE DESCRIBED HOMOGENTISIC ACID HOMOGENTISIC ACID OXIDASE –BLACK URINE –BLACK NAILS (OCHRONOSIS), SKIN –BLACK JOINT CARTILAGE (SEVERE ARTHRITIS)
- 34. NEUROFIBROMATOSIS • 1 and 2 – 1-von Recklinghausen – 2- “acoustic” neurofibromatosis • 1 – Neurofibromas, café-au-lait, Lisch nodules
- 35. NEUROFIBROMATOSIS • 1 and 2 • 1-von Recklinghausen • 2- “acoustic” neurofibromatosis • 2 – Bilateral acoustic neuromas and multiple meningiomas
- 36. MULTIFACTORIAL INHERITANCE • Multi-”FACTORIAL”, not just multi-GENIC • “SOIL” theory • Common phenotypic expressions governed by “multifactorial” inheritance – Hair color – Eye color – Skin color – Height – Intelligence – Diabetes, type II
- 37. FEATURES of multifactorial inheritance • • • • Expression determined by NUMBER of genes Overall 5% chance of 1st degree relatives having it Identical twins >>>5%, but WAY less than 100% This 5% is increased if more children have it • Expression of CONTINUOUS traits (e.g., height) vs. DISCONTINUOUS traits (e.g., diabetes)
- 38. “MULTIFACTORIAL” DISORDERS • Cleft lip, palate • • • • • • • Congenital heart disease Coronary heart disease Hypertension Gout Diabetes Pyloric stenosis MANY, MANY, MANY, MANY MORE…..
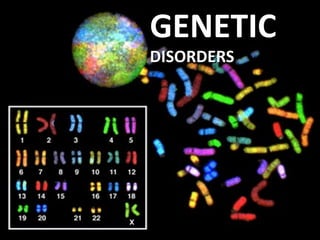
- 39. • • • • KARYOTYPING Defined as the study of CHROMOSOMES 46 = (22x2) + X + Y Conventional notation is “46,XY” or “46,XX” G(iemsa)-banding, 500 bands per haploid recognizable • Short (“p”-etit) arm = p, other (long) arm = q
- 41. More KARYOTYPING info • A,B,C,D,E,F,G depends on chromosome length – A longest – G shortest • Groups within these letters depend on the p/q ratio • ARMREGIONBANDSub-BAND, numbering from the centromere progressing distad
- 43. F.I.S.H. (gene “probes”) greatly enhances G-banding • Fluorescent InSitu Hybridization • Uses fluorescent labelled DNA fragments, ~10,000 base pairs, to bind (or not bind) to its complement
- 44. FISH • SUBTLE MICRODELETIONS • COMPLEX TRANSLOCATIONS • AND TELOMERE ALTERATIONS
- 45. TRIPLE CHROMOSOME #20 A DELETION in CHROMOSOME #22
- 47. CYTOGENETIC DISORDERS • DEFINITIONS: – EUPLOID (46XX or 46XY) –ANEUPLOID (NOT AN EXACT MULTIPLE OF 23) • MONOSOMY, AUTOSOME OR SEX • TRISOMY, AUTOSOME OR SEX – DELETION – BREAKAGE
- 48. MORE DEFINITIONS
- 49. COMMON CYTOGENETIC DISEASES • AUTOSOMES – TRISOMY-21 (DOWN SYNDROME) – 8, 9, 13 (Patau), 18 (Edwards), 22 – 22q.11.2 deletion • SEX CHROMOSOMES –KLINEFELTER: XXY, XXXY, etc. –TURNER: XO
- 50. TRISOMY-21
- 51. TRISOMY-21 • Most trisomies (monosomies, aneuploidy) are from maternal non-disjunction • (non-disjunction or anaphase lag are BOTH possible) • #1 cause of mental retardation • Maternal age related • Congenital Heart Defects, risk for acute leukemias, GI atresias • Most LOVABLE of all God’s children
- 53. Chromosome 22q11.2 Deletion Syndrome • Because of a DELETION, this cannot be detected by standard karyotyping and needs FISH • Cardiac defects, DiGeorge syndrome, velocardiofacial, CATCH*
- 55. SEX CHROMOSOME DISORDERS • Problems related to sexual development and fertility • Discovered at time of puberty • Retardation related to the number of X chromosomes • If you have at least ONE “Y” chromosome, you are male
- 56. KLINEFELTER (XXY, XXXY, etc.) • Hypogonadism found at puberty • #1 cause of male infertility • NO retardation unless more X’s • 47, XXY 82% of the time • L----O----N----G legs, atrophic testes, small penis
- 58. TURNER (XO) • 45, X is the “proper” designation • Mosaics common • Often, the WHOLE chromosome is not missing, but just part • NECK “WEBBING” • EDEMA of HAND DORSUM • CONGENITAL HEART DEFECTS most FEARED
- 60. HERMAPHRODITES ♂ ♀ • GENETIC SEX is determined by the PRESENCE or ABSENCE of a “Y” chromosome, but there is also, GONADAL (phenotypic), and DUCTAL sex • TRUE HERMAPHRODITE: OVARIES AND TESTES, often on opposite sides (VERY RARE) • PSEUDO-HERMAPHRODITE: – MALE: TESTES with female characteristics (Y-) – FEMALE: OVARIES with male characteristics (XX)
- 61. SINGLE GENE, NON-Mendelian • Triplet repeats – Fragile X (CGG) – Others: ataxias, myotonic dystrophy • Mitochondrial Mutations: (maternal) (LEBER HEREDITARY OPTIC NEUROPATHY) • Genomic “IMPRINTING”: (Inactivation of maternal or paternal allele, contradicts Mendel) • Gonadal “MOSAICISM”: (only gametes have mutated cells)
- 62. MOLECULAR DX by DNA PROBES • • • • • • • BIRTH DEFECTS, PRE- or POST- NATAL TUMOR CELLS CLASSIFICATIONS of TUMORS IDENTIFICATION of PATHOGENS DONOR COMPATIBILITY PATERNITY FORENSIC
- 63. H&E tissue structures ImmunoAntigen Proteins GENES that MAKE those PROTEINS
Notes de l'éditeur
- IMPOSSIBLE!!!!! HORROR!!!!! ANXIETY!!!!!! DREAD!!!!! INADEQUACY!!!!!
- Are ALL diseases “genetic”? Are all diseases “environmental”? How does “congenital” fit in? How does “immune” fit in? How does this fit in with DEG-INF-NEO?
- The chapter is organized in order of increasing size of the chromosomal molecular anatomic defect.
- Classical ideal concept of a point mutation, which also happens to be the REAL defect in sickle cell anemia.Why would this NOT cause a frameshift?
- In a “frameshift mutaton”, NON-multiple of three mutations “shift” the whole DNA “frame”! A frameshift mutation (also called a framing error or a reading frame shift) is a genetic mutation caused by indels (insertions or deletions) of a number of nucleotides in a DNA sequence that is NOT divisible by three!
- In the classical one-gene, one-protein model, abnormal (i.e., mutated) genes mean abnormal proteins.
- The chapter is organized in order of increasing size of the chromosomal molecular anatomic defect, from single base pair to entire chromosome!
- Each has it’s own characteristics, each has its own list of common diseases, and each has its own pedigree or pattern of inheritance
- Heterozygous ~ “less aggressive”? Single trouble?
- NOT to memorize, but be familiar with.
- Homozygous ~ “more aggressive”? Double trouble? This SHOULD make sense too?
- Most of the classical “genetic” diseases are autosomal RECESSIVE, rather than autosomal DOMINANT, by far. NOT to memorize, but be familiar with.
- Why generations skipped in AR, but not AD? Because you need defects (mutations) in BOTH alleles!
- You should know reflexively that ALL these diseases are sex linked. We will soon see a map of the X-chromosome.
- Fibrillin-1 is a major component of the microfibrils that form a sheath surrounding the amorphous elastin. It is believed that the microfibrils are composed of end-to-end polymers of fibrillin.
- The concept is extremely simple: If an enzyme cannot convert A B, then A builds up abnormally.
- You will probably never see any of these disorders personally, but nevertheless, you should have familiarity with the process behind each disease. You should already know from biochemistry what these substances are already. We will define and differentiate these groups of chemicals as we progress.
- Generic description, for more info : http://en.wikipedia.org/wiki/Glycogen_storage_disease
- Sphingolipids are a class of lipids containing a backbone of sphingoid bases, a set of aliphatic amino alcohols that includes sphingosine. “Sphingo” comes from Sphinx, because of their original enigmatic nature! Tay-Sachs disease (abbreviated TSD, also known as GM2 gangliosidosis or Hexosaminidase A deficiency) is an autosomal recessive genetic disorder. In its most common variant known as infantile Tay-Sachs disease it presents with a relentless deterioration of mental and physical abilities which commences at 6 months of age and usually results in death by the age of four.
- Sulfatides are a class of sulfated galactosylceramides synthesized primarily in the oligodendrocytes in the central nervous system. Sulfatides are a type of sulfolipid.
- Sphingomyelin (SPH), (sphin-go-my-e-lin (sfi ng gōˈmīəlin)), is a type of sphingolipid found in animal cell membranes, especially in the membranous myelin sheath which surrounds some nerve cell axons. It usually consists of phosphorylcholine and ceramide. In humans SPH represents ~85% of all sphingolipids.
- Cerebrosides are glycosphingolipids which are important components in animal muscle and nerve cell membranes. Myelin is the most well known cerebroside. Glucocerebroside (also called glucosylceramide) is any of the cerebrosides in which the monosaccharide head group is glucose. Gaucher's disease is the most common of the lysosomal storage diseases. It is caused by a hereditary deficiency of the enzyme glucocerebrosidase (also known as acid β-glucosidase). The enzyme acts on a fatty substance glucocerebroside (also known as glucosylceramide). When the enzyme is defective, the substance accumulates, particularly in cells of the mononuclear cell lineage.
- Note this is heparAn, NOT heparIn. Mucopolysaccharides Mucopolysaccharides are long chains of sugar molecules that are found throughout the body, often in mucus and in fluid around the joints. They are more commonly called glycosaminoglycans.
- Fucosidosis, also called alpha-l-fucosidase deficiency, is a rare autosomal recessive lysosomal storage disease in which the enzymefucosidase is not properly used in the cells to break down fucose. Mannosidosis is a deficiency in mannosidase, an enzyme. Aspartylglucosaminuria (AGU), also called aspartylglycosaminuria, is a rare, autosomal recessive lysosomal storage disorder caused by deficient activity of the enzyme N-aspartyl-beta-glucosaminidase (aspartylglucosaminidase). This enzyme normally cleaves long sugar chains known as oligosaccharides in the lysosome. Wolman disease (also known as Wolman's disease, Wolman's syndrome, and acid lipase deficiency) is a rare autosomal recessive lipid storage disease that is usually fatal at a very young age. It is in the family of lysosomal storage diseases. Acid Phosphate Deficiency is caused by mutations in the ACP2 (beta subunit) and ACP3 (alpha subunit) genes.
- Alkaptonuria (black urine disease or alcaptonuria) is a rare inherited genetic disorder of phenylalanine and tyrosine metabolism. This is an autosomal recessive condition that is due to a defect in the enzyme homogentisate 1,2-dioxygenase (EC 1.13.11.5), which participates in the degradation of tyrosine.
- Endogenous pigment looking like ANY other endogenous pigment, e.g., hemosiderin, melanin, bile, lipofucsin
- Neurofibromatosis (commonly abbreviated NF) is a genetically-inherited disease in which the nerve tissue grows tumors (i.e., neurofibromas) that may be harmless or may cause serious damage by compressing nerves and other tissues. The disorder affects all neural crest cells (Schwann cells, melanocytes, endoneurial fibroblasts). Cellular elements from these cell types proliferate excessively throughout the body forming tumors and the melanocytes function abnormally resulting in disordered skin pigmentation.The tumors may cause bumps under the skin, colored spots, skeletal problems, pressure on spinal nerve roots, and other neurological problems.
- We are now moving the discussion up from ONE gene MULTI-genes Parts of chromosomes WHOLE chromosomes.
- If a disease or condition is scalable, rather than on or off, it is probably multigenic, or multifactorial, just part of the spectrum of HOMO-zygous diseases being HOMO-geneous, and HETERO-zygous diseases being VARIABLE.
- You might imagine that the list of “multifactorial” disorders blends in with the entire list of human diseases. Hence are “all” diseases “genetic”? This is almost an UNFAIR list, therefore NO single gene mutation can be indicted as being the cause of any of these diseases..
- The Giemsa stain, named after Gustav Giemsa, is a VERY common stain in pathology, often used to identify organisms in cells such as malaria and helicobacter, and MANY other things such as parts of cells and connective tissue. It is a VERY simple stain to do.
- The “official” notation for the normal male pattern is: “46, XY”
- Is it surprising that the “regions” of the “X” chromosome are the same as the list of sex-linked diseases? Ans: NO Have you see this list before? Ans: YES
- Awesome research technique, used often in everyday pathology too, fluorescently “labels” pieces of DNA which connect to the corresponding strand during DNA replication. In situ hybridization (ISH) is a type of hybridization that uses a labeled complementary DNA or RNA strand (i.e., probe) to localize a specific DNA or RNA sequence in a portion or section of tissue (in situ)
- FISH is POWERFULLY more sensitive, accurate, and specific, than G-banding.
- Common applications for FISH. Examples of diseases that are diagnosed using FISH include Prader-Willi syndrome, Angelman syndrome, 22q13 deletion syndrome, chronic myelogenous leukemia, acute lymphoblastic leukemia,Cri-du-chat, Velocardiofacial syndrome, and Down syndrome, but, IN GENERAL, diseases with partial or whole chromosome abnormalities.
- This technique is used to identify structural chromosome aberrations in cancer cells and other disease conditions when Giemsa banding or other techniques are not accurate enough. Each chromosome has a different color, sort of, although some of this is digital false color techniques, much in the same way, electron microscopy can generate “false” colors. This was our spectacular title page, and you have probably figured out why.
- Just about everything you can imagine geometrically which can happen to that piece of string------does!
- Maternal “nondisjunction” is the classical explanation of Trisomy 21.
- You do not have to see many trisomy-21 patients until you can recognize them very quickly and easily. There is NO way you can learn from a textbook how to recognize these patients quickly. If you KNOW one or are RELATED to one, or loved one, you NEVER fail to recognize the face without having to describe the details, i.e., pattern-recognition. MEMORIZE THIS PIC!
- 22q11.2 deletion syndrome, also known as DiGeorge Syndrome, Velo(soft palate)Cardio(heart)Facial(face) Syndrome, conotruncal anomaly face syndrome, Congenital Thymic Aplasia, Strong Syndrome, Thymic hypoplasia, and DiGeorge anomaly. It also has the mnemonic C-A-T-C-H, for : Cardiac Abnormality (especially Fallot's Tetralogy)Abnormal faciesThymic aplasiaCleft palateHypocalcemia
- Cute smiles?
- Sexuality can be defined in many ways, having at least ONE “Y” chromosome is a good definition of being male.
- “STREAK” ovaries are the rule, neck webbing and cardiac structural abnormalities are also at the top of the list.
- “Pseudo”-hermaphrodites are MUCH more common that TRUE hermaphrodites.
- The fragile X syndrome is a learning disability genetic disorder caused by a mutation of the FMR-1 gene on the X chromosome. Mutation at that site is found in 1 out of about every 2000 males and 1 out of about every 259 females. (Incidence of the disease itself is about 1 in every 4000 females.) The number of trinucleotide repeat diseases is growing every year: http://en.wikipedia.org/wiki/Trinucleotide_repeat_disorder Leber’s Hereditary Optic Neuropathy (LHON) or Leber optic atrophy is a mitochondrially inherited (mother to all offspring) degeneration of retinal ganglion cells (RGCs) and their axons that leads to an acute or subacute loss of central vision; this affects predominantly young adult males. However, LHON is only transmitted through the mother as it is primarily due to mutations in the mitochondrial (not nuclear) DNA and only the egg contributes mitochondria to the embryo. Genomic imprinting is a genetic phenomenon by which certain genes are expressed in a PARENT-OF-ORIGIN specific manner.
- My #1 peeve, is people who identify pathology with forensic pathology. It shows they have been watching WAY too much TV.
- Evolution of tumor classifications: 1) Histology 2) Immunochemistry 3) Gene micro-arrays