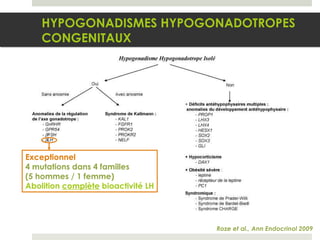
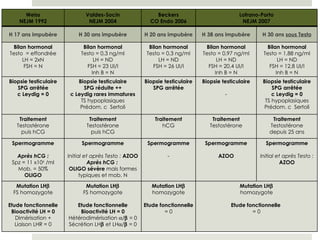
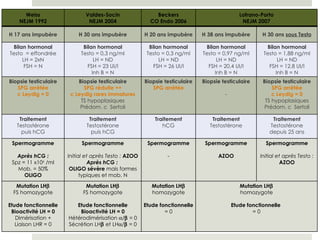
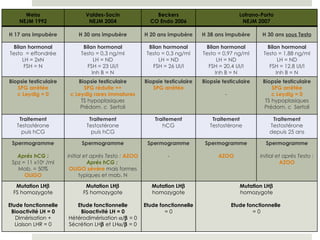
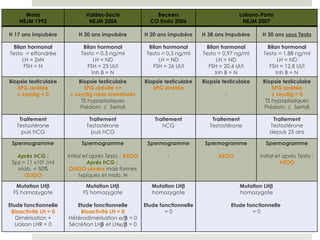
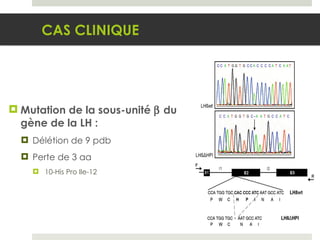
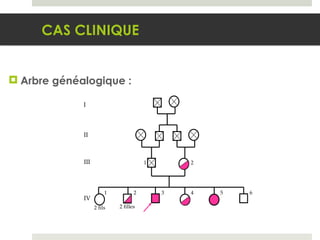
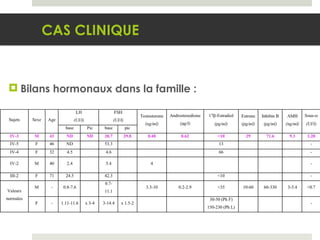
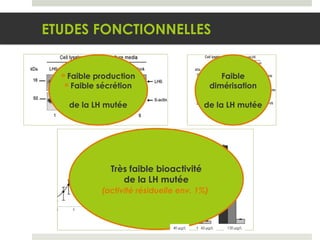
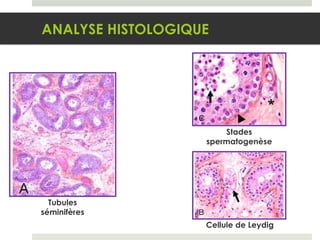
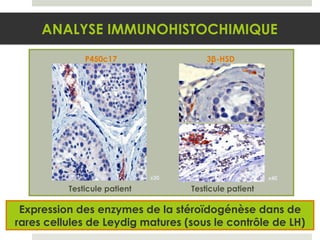
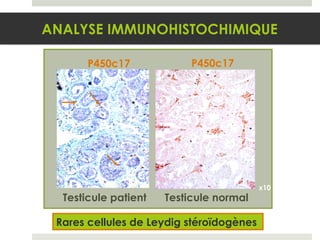
Le document présente un cas clinique d'hypogonadisme hypogonadotrope congénital chez un homme de 43 ans, diagnostic posé suite à un impubérisme à 23 ans. Les examens révèlent des anomalies hormonales et génétiques liées à une mutation de la sous-unité β de la LH, affectant la fonction des cellules de Leydig et la spermatogenèse. Divers traitements ont été tentés, montrant des impairments significatifs dans la production de testostérone et la fertilité.
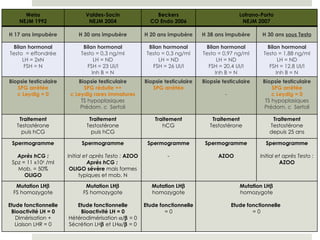
![Spermogrammes sans traitement : CAS CLINIQUE Initial Pendant 10 mois N [Spermatozoïdes] 68 x 10 6 /ml 76.4 - 127 x 10 6 /ml 40-200 x 10 6 /ml Mobilité (a+b) 20% 25% - 35% >= 50% Formes typiques 20% 5% - 23% >= 30%](https://image.slidesharecdn.com/carine-courtillot-091219095056-phpapp02/85/Carine-Courtillot-5-320.jpg)