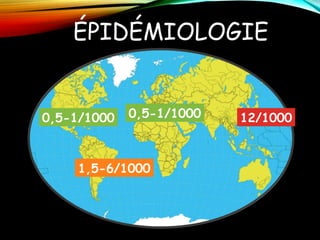
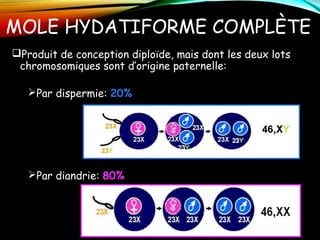
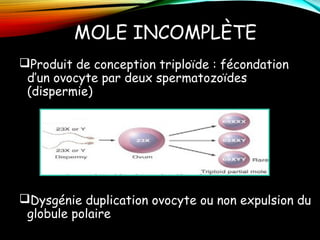
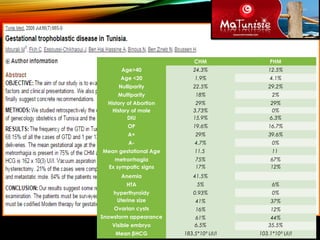
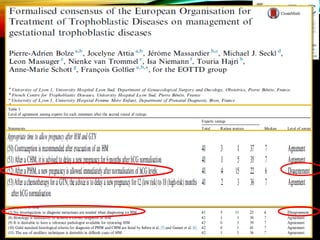
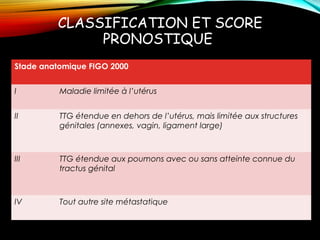
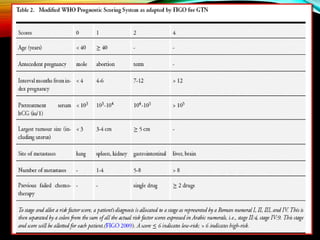
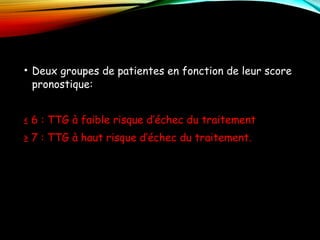
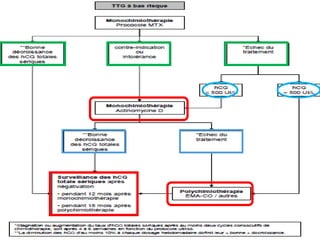
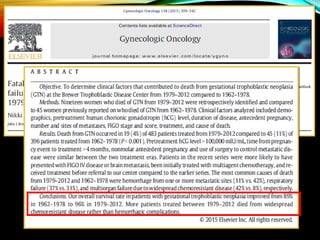
Le document traite des maladies trophoblastiques, notamment des moles hydatiformes, leur épidémiologie, facteurs de risque, diagnostic et traitement. Il présente des statistiques sur l'incidence de ces maladies et les stratégies de gestion, y compris des recommandations pour la chimiothérapie et la surveillance après traitement. Des classifications pronostiques basées sur des critères anatomiques et cliniques sont également abordées.




![Bassin obstetrical [enregistrement automatique]](https://cdn.slidesharecdn.com/ss_thumbnails/bassinobstetricalenregistrementautomatique-160906202047-thumbnail.jpg?width=640&height=640&fit=bounds)












![Kyste hydatique du foie [enregistrement automatique]](https://cdn.slidesharecdn.com/ss_thumbnails/kystehydatiquedufoieenregistrementautomatique-170224222408-thumbnail.jpg?width=640&height=640&fit=bounds)









































![Cours d immunologie generale Dr Louis [Enregistrement automatique].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/coursdimmunologiegeneraledrlouisenregistrementautomatique-260114234321-8e6b96ef-thumbnail.jpg?width=640&height=640&fit=bounds)

