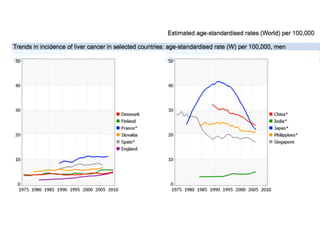
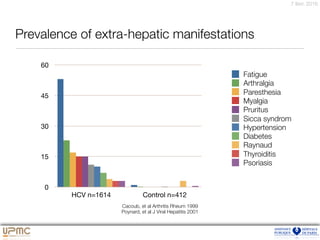
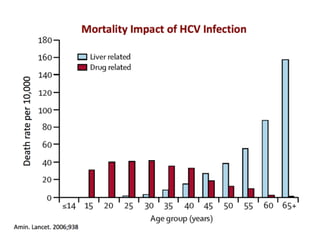
Le document présente une analyse de l'épidémiologie et de l'histoire naturelle de l'hépatite virale C, en abordant des thèmes tels que la prévalence, les facteurs de contamination, et la progression de la fibrose. Il décrit également l'impact de ces facteurs sur la mortalité et met en évidence des cas cliniques illustrant divers parcours de patients. En outre, des statistiques sur les décès lié au cancer du foie et des recommandations pour le dépistage sont également fournies.

![3,6 millions tests VHC 95%CI [3,4-3,9] en 2013: 0.9% positifs](https://image.slidesharecdn.com/plge7tet5kbciwpmdfvy-signature-b51e00367b0723c10825f3dc4b85dcf41b0c2c2d68783dc7b4ea336789ebef24-poli-160207202348/85/Histoire-hcv-du-2016-85-320.jpg)