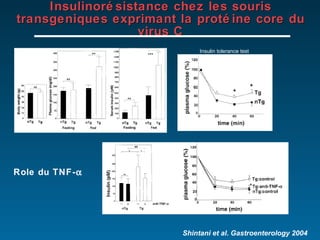
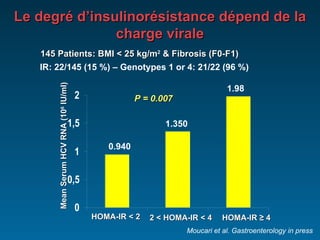
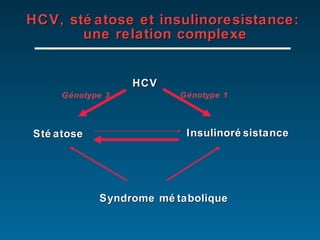
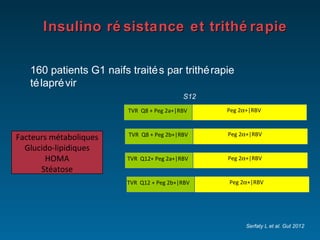
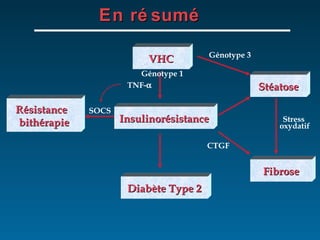
Le document examine la relation complexe entre l'hépatite C (VHC), la stéatose et l'insulinorésistance, soulignant la prévalence élevée de la stéatose parmi les patients atteints de VHC. Il discute également des facteurs de risque associés à la stéatose, en mettant l'accent sur l'importance de l'obésité et du syndrome métabolique, ainsi que sur les implications pour le traitement antiviral. Enfin, la recherche indique que la stéatose et l'insulinorésistance peuvent altérer la réponse au traitement chez les patients infectés par le VHC.


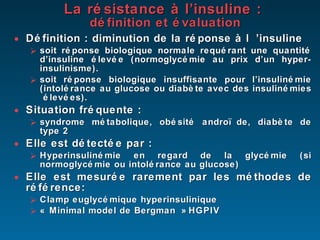
![Evaluation Formules simples mais grossières Formules mathématiques basées sur des prélèvements à jeun Homeostasis Model Assessment of Insulin Resistance HOMA : Ins (µUI/ml) x Gly (mmol/l) / 22.5 résistance à l’insuline si > 3 Quantitative Insulin Check Index QUICKI : 1 / (log [Ins (µUI/ml)] + log [Gly (mg/dl)]) HGPO : Bon compromis Formules mathématiques basées sur les prélèvements de glycémie et d’insulinémie aux différents temps de l’HGPO (0, 30, 60, 90, 120 min) Formule de Belfiore : 2/ [(AUC insulin x AUC glucose)+1] Bien corrélée au clamp](https://image.slidesharecdn.com/serfaty-du2012-120123032613-phpapp01/85/Serfaty-du-2012-6-320.jpg)





















































































































![Cours d immunologie generale Dr Louis [Enregistrement automatique].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/coursdimmunologiegeneraledrlouisenregistrementautomatique-260114234321-8e6b96ef-thumbnail.jpg?width=640&height=640&fit=bounds)