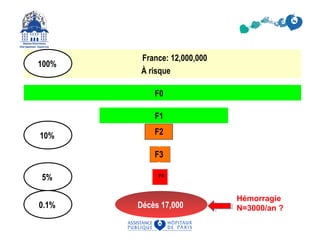
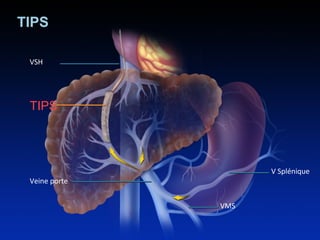
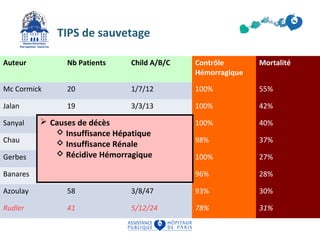
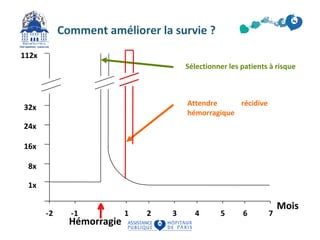
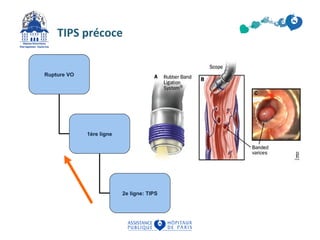
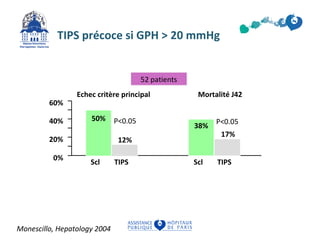
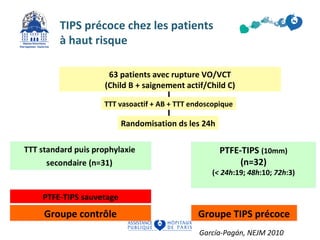
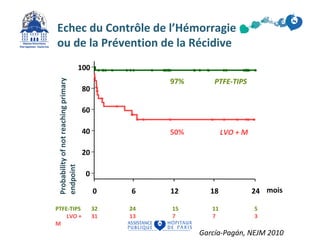
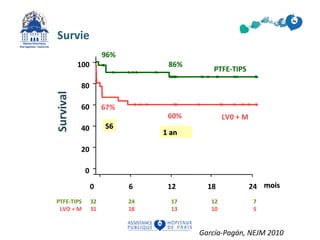
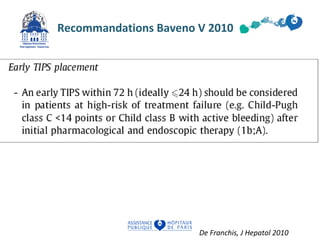
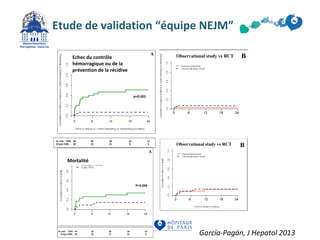
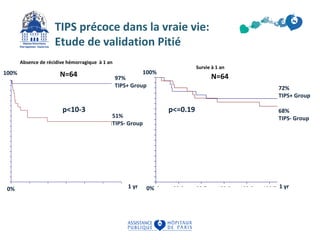
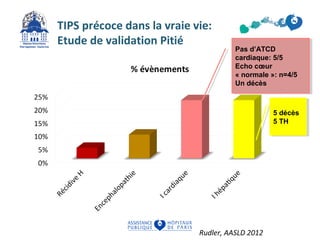
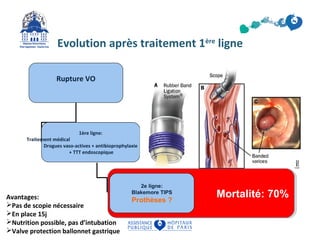


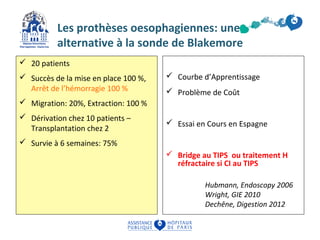


Le document traite de l'utilisation du TIPS et des prothèses oesophagiennes dans le contexte des hémorragies liées à l'hypertension portale. Il met en évidence l'efficacité du TIPS, en particulier chez les patients à haut risque, et les meilleures stratégies de traitement pour améliorer la survie. Les résultats suggèrent également une place pour les prothèses oesophagiennes comme alternative dans certains cas.























































































